TABLE 90-1 Barriers to Cancer Pain Management | |||||||
|---|---|---|---|---|---|---|---|
|
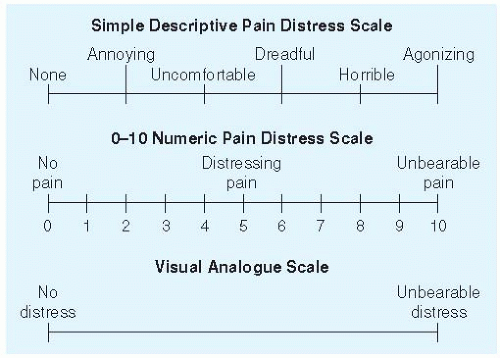 Figure 90-1 Pain assessment intensity scales. (From Jacox A, Carr DB, Payne R, et al. Management of cancer pain. Clinical practice guideline No. 9 [AHCPR publication No. 94-0592]. Rockville, MD: Agency for Health Care Policy and Research, U.S. Department of Health and Human Services, Public Health Service, 1994.) |
physical examination alone. While the workup is proceeding, any distressing pain can be treated empirically.
delivered is limited by the amount of acetaminophen in each unit dose. The risk of acetaminophen-related hepatic toxicity requires that maximal acetaminophen doses not exceed 4 g/d (<2 g/d in patients with liver disease or heavy alcohol consumption). When the maximal dose of acetaminophen is reached and pain persists, an alternative strategy for pain control is necessary.
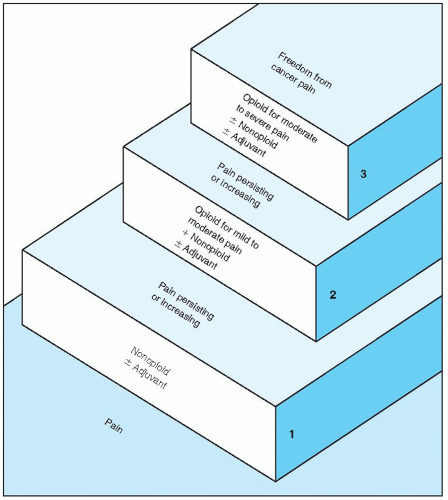 Figure 90-2 The World Health Organization’s three-step analgesic ladder. (From World Health Organization. Cancer pain relief: with a guide to opioid availability, 2nd ed. Geneva, Switzerland: Author, 1996:15, with permission.) |
TABLE 90-2 Commonly Used Analgesics and Adjuvants | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
opioid required to control pain as compared to a purely PRN regimen.
Contin, Oramorph SR, Kadian, Avinza) provides prolonged analgesia (8 to 24 hours) with less frequent dosing, but the cost can be high. These long-acting formulations cannot be crushed or chewed, but Kadian and Avinza capsules can be broken open and the contents sprinkled into food or liquid for patients who cannot swallow pills easily or are receiving tube feedings. Oxycodone is available in a long-acting, slow-release formulation (OxyContin) with an effect lasting 8 to 12 hours.
TABLE 90-3 Approximate Equianalgesic Doses of Short-Acting Opioids for Chronic Paina,b | ||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||
Related posts:
 Screening for HIV Infection
Screening for HIV Infection
 Screening for Hyperlipidemia and Associated Coronary Heart Disease Risk Factors
Evaluation of Arterial Insufficiency of the Lower Extremities
Evaluation and Prevention of Occupational and Environmental Lung Disease
Management of Chronic Obstructive Pulmonary Disease
Screening for Hyperlipidemia and Associated Coronary Heart Disease Risk Factors
Evaluation of Arterial Insufficiency of the Lower Extremities
Evaluation and Prevention of Occupational and Environmental Lung Disease
Management of Chronic Obstructive Pulmonary Disease
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


