Arterial Line Placement and Care
Khaldoun Faris
I. GENERAL PRINCIPLES
A. Cannulation sites.
1. Radial artery.
2. Dorsalis pedis artery.
3. Brachial artery.
4. Femoral artery.
5. Axillary artery.
B. Anatomy.
1. The radial artery is one of two final branches of the brachial artery. It lies just lateral to the flexor carpi radialis at the wrist (Fig. 3-1). The anastomoses between the radial and ulnar arteries provide excellent collateral flow to the hand. A competent superficial or deep arch must be present to ensure adequate collateral flow.
2. The dorsalis pedis artery runs from the level of the ankle to the great toe. It lies superficially and just lateral to the tendon of the extensor hallucis longus.
3. The brachial artery lies in the antecubital fossa, medial to the tendon of the biceps, and in close proximity to the median nerve.
4. The common femoral artery courses under the inguinal ligament near the junction of the ligament’s medial and middle thirds (Fig. 3-2).
5. The axillary artery begins at the lateral border of the first rib and ends at the inferior margin of the teres major muscle. The artery is mostly superficial and covered only by skin and fasciae.
C. Site selection.
1. The ideal artery should have extensive collateral circulation that will maintain the viability of distal tissues if thrombosis occurs.
2. The site should be comfortable for the patient, accessible for nursing care, and close to the monitoring equipment.
3. Sites involved by infection or disruption of the epidermal barrier should be avoided.
4. Larger arteries and catheters report pressures that are closer to aortic pressures. Distal artery recordings yield higher systolic values than central artery recordings, but the mean pressures are similar.
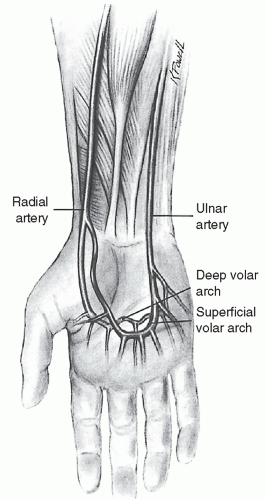 Figure 3-1. Anatomy of the radial artery. Note the collateral circulation to the ulnar artery through the deep volar arterial arch and dorsal arch. |
II. INDICATIONS
A. Hemodynamic monitoring.
1. Beat-to-beat changes.
2. Waveform inspection.
3. The effect of arrhythmia on perfusion.
4. Continuous cardiac output (CO) monitoring using arterial pulse contour analysis.
5. Assessment of systolic pressure variation (SPV), pulse pressure variation (PPV), or stroke volume variation (SVV) to predict fluid responsiveness in mechanically ventilated patients with large tidal volumes (>8 mL/kg).
B. Frequent arterial blood gas sampling (more than two measurements per day).
C. Arterial administration of drugs such as thrombolytics.
D. Intra-aortic balloon pump use.
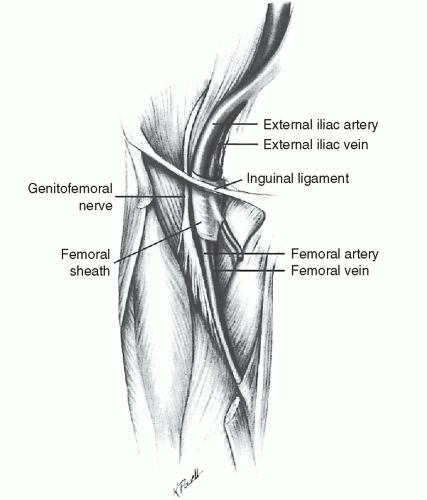 Figure 3-2. Anatomy of the right femoral artery and adjacent structures. The artery is cannulated below the inguinal ligament. |
III. PROCEDURE
A. Equipment.
1. The equipment necessary to display and measure arterial waveform includes.
a. An appropriate intravascular catheter.
b. Fluid-filled noncompliant tubing with stopcocks.
c. A transducer.
d. A device for constantly flushing the line.
e. Electronic monitoring equipment.
2. Using this equipment, intravascular pressure changes are transmitted through the hydraulic (fluid-filled) elements to the transducer, which converts mechanical displacement into a proportional electrical signal. The signal is amplified, processed, and displayed as a waveform by the monitor.
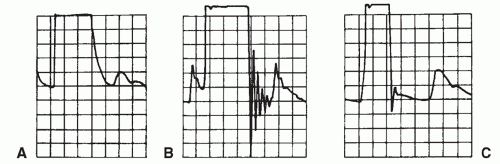 Figure 3-3. Fast-flush test. A: Overdamped system. B: Underdamped system. C: Optimal damping. |
3. Sources of error.
a. Improper zeroing of the system and zero drift are important sources of error.
b. Calibration of the system is usually not necessary because of standardization of the disposable transducer.
c. If the zero referencing and calibration are correct, a fast-flush test will assess the system’s dynamic response.
d. An optimal fast-flush test results in undershoot followed by small overshoot and then settles to the patient’s waveform (Fig. 3-3).
e. Overdamped tracings are usually caused by air bubbles, kinks, clot formation, compliant tubing, loose connections, a deflated pressure bag, or anatomic factors. All these problems are usually correctable.





