such as for a shoe (Fig. 184-2) or glove (Fig. 184-3) allergy. Patch testing can help to identify the contactant.
 Figure 184-1 Linear vesicles. This pattern is characteristic of a plant allergic dermatitis—in this case, poison ivy. |
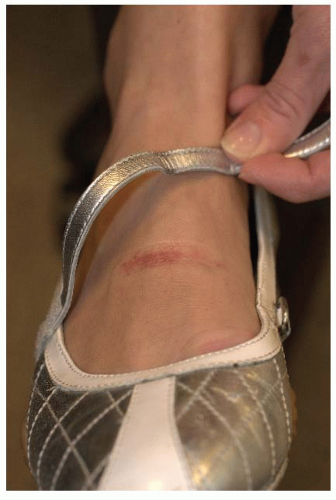 Figure 184-2 Allergic dermatitis from the chromates in tanned leather in a shoe; note dermatitis under the strap. |
 Figure 184-3 Rubber accelerator (carba and thiuram) allergic dermatitis from latex rubber work gloves. |
 Figure 184-4 Chronic irritant dermatitis from frequent handwashing. |
TABLE 184-1 Topical Corticosteroid Preparations | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Related posts:
 Screening for HIV Infection
Screening for HIV Infection
 Screening for Hyperlipidemia and Associated Coronary Heart Disease Risk Factors
Evaluation of Arterial Insufficiency of the Lower Extremities
Evaluation and Prevention of Occupational and Environmental Lung Disease
Management of Chronic Obstructive Pulmonary Disease
Screening for Hyperlipidemia and Associated Coronary Heart Disease Risk Factors
Evaluation of Arterial Insufficiency of the Lower Extremities
Evaluation and Prevention of Occupational and Environmental Lung Disease
Management of Chronic Obstructive Pulmonary Disease
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


