Approach to the Child With a Cough
Diana Lowenthal MD, FAACP
INTRODUCTION
Cough is a frequent pediatric complaint. Most episodes of coughing in children are benign and self-limited, yet families frequently are concerned that their coughing child may have pneumonia or another serious illness. In addition, coughing can interrupt a family’s sleep, disrupt the classroom, and provoke stares or comments from strangers. Health care providers who work with coughing children must be adept at discerning the cough associated with mild viral illness from that associated with a more serious malady. In addition, they must be able to reassure families that coughing is a normal part of the host defense to acute respiratory illness. This chapter will review the pertinent history, physical examination, and diagnostic evaluation of a child with a cough. In addition, it will discuss in detail the treatment of pneumonia, croup, and bronchiolitis.
ANATOMY, PHYSIOLOGY, AND PATHOLOGY
Coughing occurs in response to excess mucus secretion or the presence of foreign matter in the nasopharynx, larynx, trachea, or bronchi. The act of coughing moves mucus to the pharynx, where it can be expectorated, sneezed out, or swallowed. An effective cough requires a deep inhalation, a narrowing of the proximal airways, and then a marked, coordinated contraction of all muscles of exhalation. The process demands a profound effort, and can be affected by muscular weakness or chest or abdominal pain.
HISTORY
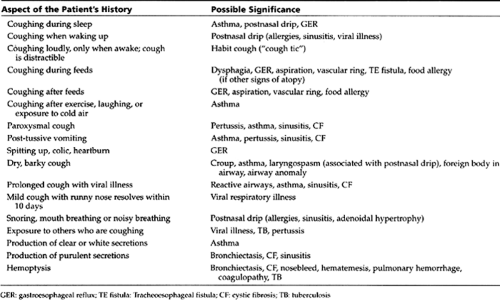
Ascertaining the nature, severity, and triggers of a cough is important. A detailed guide to important aspects of the history can be found in Table 36-1. Some general points follow.
 |
Acute or Chronic
Chronic coughing has been defined as a cough lasting for 3 weeks or more. The basic tenet is that acute coughing is likely to be a viral or self-limited process, while chronic coughing merits an evaluation for an underlying illness. This distinction, however, is not always simple. Pediatric providers must recognize the child who presents with a cough that is acute yet recurrent—not an uncommon scenario. For example, the child who develops 10 days of “acute” coughing every month still warrants an evaluation for chronic cough.
• Clinical Pearl
Children with chronic respiratory problems can present with acute respiratory illness, which may or may not be related to the underlying condition.
In a child who has chronic respiratory problems, it is extremely helpful to ask the parent: “Is this the same type of cough your child usually gets with asthma (or allergies, sinusitis, etc.), or is the cough different this time?” It is helpful to see if a pattern to the cough exists and how it fits into the child’s overall health history. Regardless of the duration of the cough, providers must use good clinical judgment to evaluate the severity of the illness.
Timing
Ascertaining the time of day that the cough is most severe is one of the most important and helpful tasks. Coughing from postnasal drip can occur at any time but tends to be most prominent when the child first wakes up in the morning. It also may be troublesome when the child first lies down. Bronchospasm is likely to cause a cough that is most annoying in the middle of the night; however, postnasal drip, pertussis, and gastroesophageal reflux also strike at night. On the contrary, the cough that occurs all day—especially during times of stress—yet disappears completely the instant the child falls asleep, may be a habit cough, also called a cough tic or psychogenic cough.
Seasonal Pattern
In temperate climates, coughing is a far more common complaint during the winter, especially in those with viral respiratory illnesses, asthma, or sinusitis. Bronchiolitis from respiratory syncytial virus (RSV) usually occurs between October and March but can happen at other times as well. A pattern of coughing in the fall, spring, or both should raise suspicions about allergic rhinitis and allergy-triggered asthma.
Sound
Families and providers often point out the nature of the cough, using terms such as dry, moist, loose, tight, barking, honking, or hacking. This element of the history can be helpful but usually is not specific enough to help pin down the diagnosis. Some practitioners have come to label all children with a dry, barking cough as having “croup”. This practice should be avoided unless one is explicitly referring to a specific acute viral illness characterized by inspiratory stridor. Patients diagnosed as having “recurrent croup” are likely to have asthma, postnasal drip, or sinusitis.
Coughing fits, or paroxysms, often followed by post-tussive vomiting are common in patients with pertussis. Similar coughing fits can occur in patients with asthma, bronchiolitis
and other viral infections, sinusitis, and cystic fibrosis (CF).
and other viral infections, sinusitis, and cystic fibrosis (CF).
A loud, brassy cough is seen in patients with cough tic (a habit cough) or tracheomalacia. Many patients with residual tracheomalacia associated with tracheoesophageal fistula will have a troublesome brassy cough. Patients with asthma will often report a change in cough from dry to wet (or tight to loose) as they improve.
Relationship to Feeding
Coughing that is triggered primarily by food intake always warrants evaluation. These patients may develop aspiration, laryngospasm, choking, or apnea. Newborns with suck-and-swallow incoordination may cough and sputter upon initiation of feeds, perhaps accompanied by oxyhemoglobin desaturation, cyanosis, or apnea. Patients with neuromuscular disease may have varying degrees of dysphagia, most commonly presenting with respiratory difficulty when drinking thin liquids. Infants or young children with coughing or choking during feeding and a history of stridor or wheezing may have a vascular ring. Babies with an H-type tracheoesophageal fistula may present with aspiration episodes and abdominal distension from swallowing air. Gastroesophageal reflux (GER) may occur at any age but is most likely to elicit respiratory symptoms in infants. The child may cough, choke, or have apnea toward the end of a feed or even an hour or longer afterward. Choking, nasal congestion, arching of the back, drooling, hoarseness, and irritability may characterize the event. The child may appear to be in pain or seem to have a bad taste in the mouth. If there is associated laryngospasm, bronchospasm, or aspiration, the child may have respiratory distress. The diagnosis of GER is more likely when these symptoms occur in association with vomiting.
Some infants with prominent respiratory symptoms from GER have reflux up to the larynx or pharynx only and may never actually display significant vomiting. They are essentially “spitting up internally.”
Finally, children with coughing during feeds accompanied by signs of allergy (eg, rhinitis, conjunctivitis, puffy eyelids, eczema, hives, or wheezing) may have an underlying food allergy. Food allergy is seen most commonly in infants and young children.
Past Health History
Clues to the etiology and significance of the cough may be found in the patient’s personal or family health history or in the environment. Has the child presented with coughing before? If so, what was the cause and what worked to make it better? Equally important, which medications were tried in the past for coughing and did not work? Does the child generally wheeze or go into respiratory distress after the onset of coughing? Does the child have a history of asthma, allergies, or sinusitis?
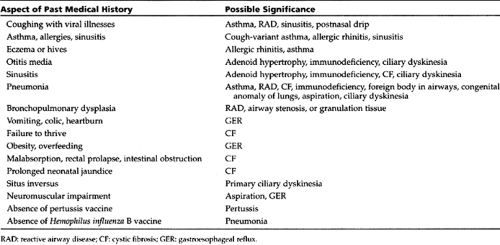
The child’s past medical patterns are important. It is alarming when a child who was never prone to respiratory problems in the past begins to have such symptoms. While this scenario may only indicate the late onset of asthma or allergies, it also can be the presentation for a collagen vascular disease or an airway tumor. While most providers will consider CF in the child with a cough, failure to thrive, and malabsorption, it is important to remember that CF is quite variable. Ten percent of
patients with CF do not have malabsorption, and some patients with CF are overweight. Table 36-2 lists some important aspects of past medical history and their implications.
patients with CF do not have malabsorption, and some patients with CF are overweight. Table 36-2 lists some important aspects of past medical history and their implications.
 |
Family History
Most children with asthma have a positive family history. Uncovering a family history of asthma can be trickier than it seems, however, as many patients are undiagnosed or have been mislabeled as having various forms of chronic or recurrent “bronchitis.” Siblings may have been diagnosed with “recurring croup.” Display 36-1 lists important aspects of the family history to explore.
DISPLAY 36–1 • Pertinent Family History
Asthma, bronchitis, chronic cough, use of inhalers
Allergies (environmental or food), eczema, hives
Sinusitis
Cystic fibrosis
Ciliary dyskinesia
Heartburn, gastroesophageal reflux
Tuberculosis
Histoplasmosis or other fungal illness (in endemic areas)
• Clinical Pearl
Providers should ask the following questions:
Does anyone in the family have a history of severe or prolonged coughing when they have a cold, wheezing, or “having things go to their chest” easily?
Does anyone in the family use an inhaler, puffer, or nebulizer machine?
Environmental History
The environmental history should include the home, neighborhood, school, daycare center or babysitter’s home, as appropriate. It also should include the work site of employed adolescents. If the parents are divorced, there may be two home environments to consider. It is gratifying to cure a chronic cough by making appropriate modifications to the home environment. Display 36-2 lists important aspects of the environmental history.
DISPLAY 36–2 • Clues in the Environment
Pets or farm animals
Cigarette smoke
Mildew, dampness (especially bathroom, basement, roof, haystacks, stable)
Dust (cluttered rooms, stuffed animals, construction, renovation)
Fumes
Wood-burning stove
Cockroaches
Occupational exposures (for employed adolescents)
PHYSICAL EXAMINATION
The office examination can help pinpoint whether the cough is from the upper or lower airway, or both. It is an ideal opportunity for noting the severity and character of the cough. Although time consuming, reproducing the cough in the office, perhaps by having the child perform some exercise or watching the infant feed, can be extremely revealing.
Initially, providers should observe the patient from afar for signs of respiratory distress, tachypnea, pallor, cyanosis, retractions, or nasal flaring. They should try to perform physical examination of the chest with the child quiet and relaxed. For infants and toddlers, the parents should hold the child comfortably in their arms. Providers should auscultate the chest carefully for the presence, quality, and symmetry of breath sounds. They should listen for adventitious
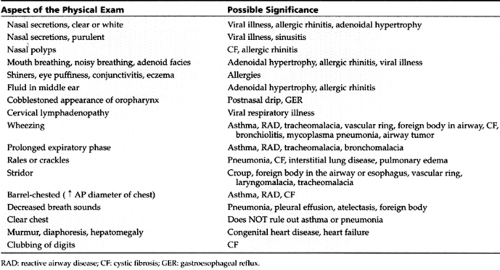
sounds: rales, ronchi, and wheezes. A particularly important portion of the respiratory cycle is the end of inspiration, during which fine rales are common. Table 36-3 lists some notable aspects of the physical examination.
sounds: rales, ronchi, and wheezes. A particularly important portion of the respiratory cycle is the end of inspiration, during which fine rales are common. Table 36-3 lists some notable aspects of the physical examination.
 |
• Clinical Pearl
Clinicians also should focus on the inspiratory to expiratory (I:E) ratio. The expiratory phase is commonly prolonged in children with reactive airway disease or asthma and may be the only positive finding on exam.
DIAGNOSTIC CRITERIA
In the vast majority of cases, providers will establish the correct diagnosis based on the findings of the history and physical exam. Additionally, the patient’s age will affect the various diagnostic considerations, as certain diagnoses tend to be more age-specific than others.
In young infants, coughing can be a sign of congenital anomaly, such as tracheomalacia, a vascular ring, pulmonary sequestration, or tracheoesophageal (TE) fistula. In addition, GER commonly presents in young infants. Providers also should consider chlamydia pneumonitis in young infants with a cough, eye discharge, or otitis media.
While toddlers are prone to laryngotracheobronchitis (croup) from parainfluenza virus, adenovirus, or RSV, providers should consider aspiration of a foreign body as well, especially when the onset of symptoms is particularly abrupt. Children in daycare and school-age children share numerous respiratory ailments, such as viral illnesses, mycoplasma pneumonia, and even tuberculosis (TB).
Adolescents with waning pertussis titers, children who did not receive pertussis vaccine, and infants awaiting vaccination are all at risk for weeks of severe coughing spasms if they contract whooping cough. Additionally, providers should ask preteens or teens with chronic cough if they smoke.
DIAGNOSTIC STUDIES
Most children with a cough require no diagnostic testing. Providers should initiate an evaluation if the cough is persistent, frequently recurring, or severe. Evaluation should proceed in a stepwise fashion, depending on the probable yield and risk of the test. The most basic tests should include a chest x-ray and a complete blood count with differential.
Imaging Studies
When ordering a chest radiograph, it is important to order films in both the posterior–anterior (PA) and lateral positions. It is not uncommon to miss findings if only the PA film is ordered. It is always worthwhile to provide the radiologist with clinical information. The chest x-ray may reveal pneumonia, an unsuspected aspirated foreign body, bronchiectasis in a patient with CF, or lymphadenopathy suggestive of TB. Commonly, the chest x-ray may reveal signs of hyperinflation or atelectasis as a result of mucus plugging, findings suggestive of bronchiolitis or asthma. Peribronchial cuffing or central perihilar densities also suggest asthma. The x-ray also may detect pleural disease, interstitial disease, pulmonary edema, congenital pulmonary anomalies, or a mass. If a mass is detected, a chest CT may be useful in further delineating the lesion. Serial radiographs can be helpful in determining whether or not an abnormality is persistent.
Localized hyperinflation suggests an endobronchial foreign body. In such cases, decubitus films, or, in cooperative older children, inspiratory and expiratory films may be ordered to enhance findings of unilateral hyperinflation secondary to a retained foreign body. A mucus plug in the airway due to asthma or bronchiolitis may yield the same radiographic appearance as a foreign body. If the clinical history is suggestive, and there is no history of foreign body aspiration, the provider may elect to treat for asthma and repeat the chest x-ray to see if the localized hyperinflation has disappeared.
A normal chest radiograph can give reassurance, narrow the diagnostic possibilities, and reduce the use of unnecessary antibiotics.
A normal chest radiograph can give reassurance, narrow the diagnostic possibilities, and reduce the use of unnecessary antibiotics.
A soft tissue x-ray of the neck can reveal adenoidal hypertrophy or various forms of upper airway obstruction. Sinus films may detect air-fluid levels or opacification, but a sinus CT scan has greater sensitivity for sinus disease and anatomy.
The upper gastrointestinal (GI) series, or barium swallow, is helpful in the child with cough related to feedings. It is less sensitive in detecting GER as the pH probe but can detect associated anatomical problems, such as hiatal hernia, and is very sensitive for cases of vascular ring. Finally, an upper GI series can sometimes detect an H-type tracheo-esophageal fistula, although these are notoriously difficult to find. For obvious reasons, a technician and radiologist accustomed to performing this study on infants and young children should perform the GI series.
A modified barium swallow, or cinefluoroscopy, is helpful in the evaluation of the child who may be aspirating oral feedings. In this study, the patient eats and drinks barium-coated drinks and foods in various textures. Fluoroscopy is performed while the child swallows, so that abnormalities in the swallowing mechanism and any tracheal aspiration can be documented.
Laboratory Evaluation
The complete blood count (CBC) may reveal an elevated number of eosinophils in patients with asthma, allergies, or chlamydia. Neutrophils will be elevated in bacterial pneumonia, sinusitis, or CF, and lymphocytes will be high in viral illness or pertussis. Quantitative immunoglobulins (IgG, IgA, and IgM) may be useful to measure in the patient with recurring cough and frequent infections. The quantitative subclasses of IgG also can be determined, but there is significant variability in the reliability of results from different laboratories. Serum IgE can be measured to detect allergies. Blood cultures can occasionally establish the etiology of bacterial pneumonia.
Testing for Cystic Fibrosis
Currently, three states perform CF screening in all newborns, and several other states are considering initiating these programs. Elsewhere, testing is ordered when providers suspect the condition. The most sensitive test is the sweat test, which should be ordered whenever a child has a history of repeated lower respiratory infections with or without malabsorption or failure to thrive. Whenever possible, providers should choose a laboratory with extensive experience and credentials for performing the sweat test, such as a Cystic Fibrosis Foundation–accredited laboratory. Genetic testing (mutation analysis) has lower sensitivity, depending on the particular laboratory and the patient’s ethnic background. The reader should refer to Chapter 55 for more information about CF.
Allergy Testing
Children with a cough from asthma, rhinitis, or sinusitis often have underlying allergies. In the past, referral for allergy testing and desensitization was almost a knee-jerk reaction to a diagnosis of asthma. Today, it is clear that allergy testing and desensitization demonstrate very limited utility for children with asthma. They may be moderately useful for youngsters with allergic rhinitis unresponsive to medical therapy with nonsedating antihistamines and intranasal steroids.
Testing may be warranted in certain situations, such as when the family needs evidence that a family pet is causing the problem or if food allergies are suspected. Skin tests have the greatest sensitivity in detecting allergies. Specific IgE radioallergosorbent technique (RAST) tests are less sensitive and more expensive, particularly if a large panel of tests is requested. Skin or RAST tests should check for the most likely allergens related to the patient’s environmental exposures and seasonal pattern of illness. In young infants, foods are the most likely allergens; the likelihood of environmental allergies increases with age.
Mantoux (Tuberculin) Testing
A reliable method of tuberculin testing, such as the Mantoux (PPD) test, is a basic part of the evaluation of coughing children. This testing becomes more important if there is a history of exposure, suggestive findings by radiograph, or any documented pneumonia.
MANAGEMENT: GENERAL PRINCIPLES
Treatment of the cough will clearly depend upon the etiology, which is not always apparent upon initial presentation. The most common cause of cough is postnasal drip associated with a viral illness. No medical treatment is mandated if the child is breathing, feeding, and sleeping comfortably. Providers should educate families that not all coughing requires medicine.
If the cough is severe or persistent, initial treatment approaches should reflect the most common etiologies: bronchospasm, rhinitis, or sinusitis, or associated with a viral illness or allergies. While pursuing a diagnostic evaluation, as described above, it is reasonable to give a trial of bronchodilators if asthma is the suspected etiology. If sinusitis is suspected and the symptoms have persisted for at least 7 to 10 days, a course of antibiotics may be useful.
Providers should minimize the use of cough suppressants. They should explain to families that cough is a normal part of the body’s defense against viral illness. If a cough is severe enough to warrant treatment, it is preferable to treat the cause of the cough, such as nasal congestion, bronchospasm, or sinusitis. A rare dose of a cough suppressant, such as dextromethorphan or a mild codeine preparation, may allow an exhausted family to get some sleep. If a child requires more than a rare dose of cough suppressant, however, an evaluation to find out the root of the cough is needed. Cough suppressants should be avoided in patients with impaired mucociliary clearance, asthma, pertussis, or CF. Narcotics, such as codeine, should be avoided in patients with significant snoring, upper airway obstruction, or chronic lung disease, as they can worsen ventilation. Expectorants, found in numerous over-the-counter cold and cough medications, are not effective in relieving cough.
In a child with cough secondary to allergic rhinitis, a trial of antihistamines is often very helpful, both in treating the symptoms and “confirming” that an allergy is likely. Control or containment of common environmental allergens may also be useful. Perennial symptoms may reflect dust mite, cockroach, or pet allergy. Simple maneuvers such as keeping furry pets out of the child’s bedroom, minimizing stuffed animals and other dust collectors, and encasing the bedding may also be beneficial.
SPECIFIC CAUSES OF COUGH
No discussion of cough in children would be complete without a brief discussion of upper respiratory infections (URIs), asthma (also termed reactive airway disease), and bronchitis. Croup, bronchiolitis, and pneumonia are discussed in greater detail in the sections that follow.
Upper Respiratory Infection
By far, the most common etiology for a cough in an otherwise healthy child is an acute respiratory viral illness. The cough in this case is the result of postnasal drip and mucus hypersecretion. The afflicted child may develop a runny or stuffy nose, perhaps some fever, and cough. Generally, the cough is not severe, and the child has minimal interruption in sleep or other daily activities. The child may appear well or only mildly ill. The chest examination will be normal. Often, other family members will be affected as well. The cough generally resolves itself within 10 days and requires no specific treatment. If the fever persists for several days or if the child appears ill or has a marked loss of appetite or persistent vomiting, the provider must consider the possibility of pneumonia, even if the examination is normal.
Asthma/Reactive Airway Disease (RAD)
If the cough is disturbing the child’s sleep or associated with post-tussive vomiting, providers should consider the possibility of asthma or reactive airway disease (RAD). This is true even if the child is not wheezing.
A common error is to dismiss the possibility of RAD or asthma in a child whose chest exam is clear. Many times, children with these conditions may not wheeze.
Infants cannot cooperate in taking a deep breath for chest examination, so providers may miss mild wheezing on auscultation. They also can miss wheezing on examination of a screaming, fussy baby. Children may wheeze mainly at nighttime and sound completely clear during the day. Many children with RAD present with a cough and perhaps coarse breath sounds and a prolonged expiratory phase, but no overt wheezing. Finally, patients with severe bronchospasm may not be moving enough air to generate a wheeze.
Young children often show evidence of airway reactivity with nearly every viral respiratory illness. If the cough is disturbing to the patient and family or does not clear up after 10 days, a trial of asthma medications (eg, a bronchodilator, perhaps with a short course of an oral corticosteroid) may be warranted. Another option, if nasal congestion is prominent, is to try a decongestant or antihistamine. Coughing that restricts a child’s sleep, activity, or school attendance and prevents parents from attending work is worth treating. A more detailed discussion of asthma and cough-variant asthma is presented in Chapter 55.
Bronchitis
Bronchitis, defined as inflammation of the bronchial epithelium, occurs as part of the clinical spectrum of many different diseases. As such, its existence as an isolated illness is unusual during childhood. Most children who are experiencing bronchial inflammation have antecedent or current viral illness. Inflammation and spasm of the bronchi also occur as part of the spectrum of asthmatic illness. Bordatella pertussis, measles, influenza and diphtheria, can all involve the tracheobronchial airway and as such produce the harsh cough that is observed with inflammation of this part of the respiratory tree. With croup, a relatively common illness in early childhood, there is inflammation of the trachea, bronchi, and larynx. (Please refer to the ensuing discussion of croup.) Environmental allergens, irritants, pollutants, and toxins can also affect the bronchi and cause acute or chronic symptoms.
History and Physical Exam
The usual course of viral bronchitis begins with nasal congestion and rhinitis, followed by a cough. Low-grade fever may be present. Initially, the cough is dry and hacking, causing significant retrosternal discomfort as it progresses. After several days of a dry cough, a wet and productive cough with purulent sputum follows. This thick sputum begins to thin at about the 10th day of illness, with steady resolution of the cough. Most children and adults can expect resolution of all symptoms within 2 weeks from the start of symptoms.
Auscultation of the chest may reveal coarse breath sounds, ronchi, and rales. The cough may persist briefly after all mucus is cleared. For most children, the cough and discomfort that it causes become the prominent symptoms and complaints.
Diagnostic Criteria
Findings gleaned from the history and physical exam usually establish the diagnosis. Viral illnesses and the spectrum of RAD/asthma account for the vast majority of cases. More rarely, anatomical or functional problems of the airways cause a persistence of or recurring pattern of symptoms of bronchitis. Providers should consider ciliary dyskinesias, bronchiectasis, TB, and CF in patients whose symptoms do not resolve or are recurrent. They also should rule out a foreign body or local or systemic immune deficiency. In older children and adolescents, providers must consider cigarette smoking, marijuana use, and inhalation of noxious gases (eg, from spray cans) as possible causes of ongoing or frequently recurring symptoms.
Management
Although Streptococcus pneumonia, Moraxella catarrhalis and non-typeable Haemophilus influenza may cause superinfection of the bronchi, antibiotics generally have not been found to be useful in producing a speedier resolution of symptoms. Antihistamines and decongestants have also not been proven helpful in relieving symptoms. Coexisting illness such as sinusitis or pneumonia may contribute to or be complications of bronchitis. Lack of resolution of symptoms after 10 to 14 days should prompt consideration of these conditions.
• Clinical Pearl
In a normal child, bronchitis as an entity for which to prescribe antibiotics does not exist. There is little justification for the practice of treating otherwise healthy children with antibiotics for bronchitis.
Immunocompetent children with normal mucociliary function do not develop bacterial bronchitis. On the other hand, antibiotics certainly have a role for children with pneumonia, sinusitis, or CF.
Viral Croup (Laryngotracheobronchitis)
Croup is technically a syndrome, the hallmark of which is upper airway obstruction and stridor. Congenital airway anomalies, smoke inhalation, postintubation stridor, measles, and diphtheria can all cause a croup syndrome. In common parlance, however, the term croup refers to the most frequently occurring variety, laryngotracheobronchitis (LTB), or viral croup. While most children with LTB have mild illnesses that can be treated at home, the potential exists for severe airway obstruction or even respiratory failure.
Pathology
Viral infection of the airways produces inflammation and edema of the larynx, trachea, and bronchi, which clinically manifests as hoarseness, stridor, and coughing respectively. The pathology is primarily subglottic, as opposed to the now rare condition of epiglottitis in which the pathology is supraglottic. Clinically there is primarily upper airway obstruction, with variable degrees of lower airway obstruction.
Epidemiology
Croup is seen most commonly in children ages 6 months to 3 years, with peak incidence between ages 1 and 2 years. It is more common in males. When the clinical features of croup are seen in an infant younger than age 6 months, providers should consider the possibility of a congenital airway anomaly.
Parainfluenza virus is the most common cause of croup, but RSV, adenovirus, and influenza virus are also possibilities. Cases appear throughout the year, but peak in the fall and spring. Reinfection can occur but is generally milder. Croup is diagnosed in 1.5% to 4.7% of 1-year-olds, based on reports from two American pediatric practices (Foy, et al., 1973; Denny, et al., 1983).
History and Physical Exam
The illness begins with a brief prodrome of a runny nose, perhaps accompanied by a low-grade fever. Next, symptoms develop related to airway edema: a loud, barking, hoarse-sounding cough; and inspiratory stridor. These problems often start quite suddenly, most commonly at night. In more severe cases, marked retractions, particularly sternal, may occur. Stridor may be noted when the child is crying or excited, but in more severe cases it may be present even at rest. There also may be expiratory wheezing. In mild cases the child feeds well, appears comfortable, and plays normally. In moderate cases, the stridor is more pronounced, and the child may appear somewhat uncomfortable, as if the throat is irritated from speaking or coughing. In severe cases, the child may have tachycardia and tachypnea and appear anxious and uncomfortable associated with decreased activity and poor feeding. Pulse oximetry may reveal hypoxemia on the basis of hypoventilation and mucus plugging, which is always a worrisome sign. The child with stridor and retractions at rest has significant airway obstruction. Younger children, having a narrower airway, are most severely affected.
Diagnostic Criteria
The diagnosis of croup is made clinically; its features, however, often overlap with those of other conditions causing stridor and dry cough (eg, foreign body aspiration, congenital airway anomaly, laryngospasm associated with allergies, or postnasal drip). Providers should suspect older patients with a barky cough or any patient with “recurrent croup” of having asthma, allergies, or postnasal drip. The term “recurrent croup” is a description, not a diagnosis. Epiglottitis is in the differential diagnosis but has become rare in the era of Haemophilus influenza B vaccination. While epiglottitis can cause the sudden onset of stridor and respiratory distress, it generally does not produce significant hoarseness or cough.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


