 Figure 235-1 Past month use of selected illicit drugs among persons aged 12 or older: 2002-2011. Findings from National Survey on Drug Use and Health, SAMHSA. |
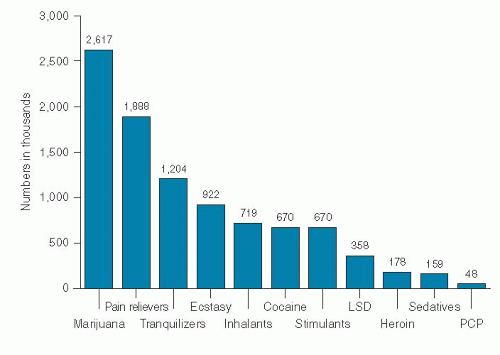 Figure 235-2 Past year initiates of specific illicit drugs among persons aged 12 or older: 2011. Findings from National Survey on Drug Use and Health, SAMHSA. |
 Figure 235-3 Source where pain relievers were obtained for most recent nonmedical use among past year users aged 12 or older: 2010-2011. Findings from National Survey on Drug Use and Health, SAMHSA. |
 Figure 235-4 Rates of opioid pain reliever (OPR) overdose death, OPR treatment admissions, and kilograms of OPR sold—United States, 1999-2010. The Centers for Disease Control and Prevention Report. |
When abused, these medications are taken orally, crushed, and snorted or used intravenously.
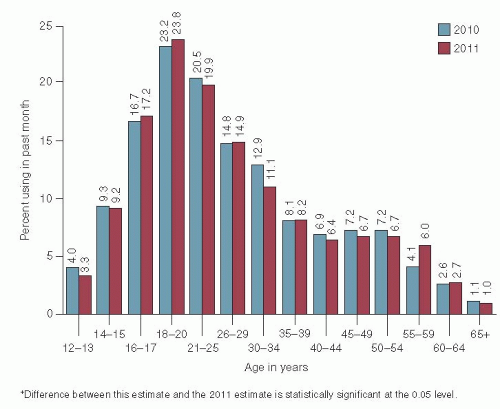 Figure 235-5 Past month illicit drug use among persons aged 12 or older, by age: 2010 and 2011. Findings from National Survey on Drug Use and Health, SAMHSA. |
of euphoria. They affect breathing, blood pressure, and arousal and also have antitussive and antidiarrheal properties.
TABLE 235-1 The Population at Increased Risk of Developing Drug Use Disorders | ||
|---|---|---|
|
TABLE 235-2 Diagnostic Criteria for Substance Use Disorders* | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
with repeated consumption, increasing doses are required to achieve the desired euphoria. Tolerance to the respiratory depressant effects of opiates develops approximately in parallel. Tolerance to opiate-induced pupillary constriction does not develop.
 Figure 235-6 From 2010 SAMHSA/CSAT Methadone Mortality Meeting, July 2010. |
Related posts:
 Screening for HIV Infection
Screening for HIV Infection
 Screening for Hyperlipidemia and Associated Coronary Heart Disease Risk Factors
Evaluation of Arterial Insufficiency of the Lower Extremities
Evaluation and Prevention of Occupational and Environmental Lung Disease
Management of Chronic Obstructive Pulmonary Disease
Screening for Hyperlipidemia and Associated Coronary Heart Disease Risk Factors
Evaluation of Arterial Insufficiency of the Lower Extremities
Evaluation and Prevention of Occupational and Environmental Lung Disease
Management of Chronic Obstructive Pulmonary Disease
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


