Figure 21.1
Patient positioning during a laparoscopic appendectomy. The patient is placed on the operating room table in the supine position with the right arm abducted to facilitate intravenous axis and the left arm tucked against the body to allow room for the surgeon and assistant to stand
General endotracheal anesthesia is the preferred method of anesthesia. Deep vein thrombosis prophylaxis should be administered prior to induction as either sequential compression devices, unfractionated heparin, or low molecular weight heparin [18]. A Foley catheter may be placed to monitor fluid status and an orogastric tube may be placed to decompress the stomach. This is particularly important if we access the abdomen using a Veress needle in the left upper quadrant because it allows decompression of the stomach and minimizes the likelihood of gastric injury.
Open Appendectomy: Procedure Description
Abdominal Access
A 2–6 cm incision is made at McBurney’s point; a Rocky-Davis (i.e. transverse) or a McBurney (i.e. parallel to the external oblique muscle) incision can be used. The location of the incision may be made at a slightly different point depending on location of maximum tenderness on palpation prior to anesthesia or if there is a palpable mass. An alternative and less commonly performed incision is a lower midline, which may facilitate exposure if the patient is obese or assist in exploration of the pelvis if the operating surgeon suspects underlying pelvic pathology.
Identification of Appendix
The incision is carried down to the external oblique which is incised parallel to its fibers. The internal oblique is then bluntly separated exposing the transversus abdominus and underlying transversalis fascia, which is then divided. The peritoneum is exposed, lifted and incised, opening a window into the peritoneal cavity. The appendix and cecum are identified and mobilized anteriorly toward the wound. To do this, it is often necessary to sharply or bluntly mobilize the cecum and terminal ileum away from their retroperitoneal attachments. If the appendix cannot be located, the surgeon can identify the taenia coli of the cecum and track them down to the base of the appendix.
Ligation of Mesoappendix
The mesoappendix is usually ligated first to avoid appendiceal artery injury during excision of the appendix. The mesoappendix and adjoining appendiceal artery may be ligated with a non-absorbable suture and then divided, or alternatively transected with a GIA or TA stapler.
Ligation of Appendix
We prefer to resect the appendix by initially crushing it at the base with a clamp followed by a suture ligature. A purse-string suture is then placed in the cecum surrounding the base of the appendix. The appendix is divided just beyond the suture ligature. Electrocautery may be used to cauterize the appendix with the intention of preventing a mucoceole. The appendiceal stump is inverted into the cecum and the purse-string suture secured to invert the appendiceal base. An alternative to using a suture ligature to remove the appendix is to transect the appendix with a GIA or TA stapler.
Inspection and Closure
Once the appendix and mesoappendix are removed from the operative field, hemostasis is ensured and the right lower quadrant inspected. If spillage is present, the area is aspirated and irrigated with several liters of normal saline. The peritoneum and transversalis fascia are closed with a running suture followed by closure of the internal oblique with another running suture. The external oblique fascia is closed with a running suture. The subcutaneous tissue is closed with interrupted sutures. The skin is closed with subcuticular sutures and then with either steri-strips or topical skin adhesive. The skin is typically left open if the appendix is perforated.
Laparoscopic Appendectomy: Procedure Description
Abdominal Access
There are numerous ways to gain access into the intraperitoneal cavity. In a non-obese patient, we prefer to access the intra-abdominal cavity by the Hasson technique. A transverse curvilinear incision is made below the umbilicus followed by blunt dissection to the midline fascia and umbilical stalk. The umbilical stalk is then grasped at its base and elevated. An approximately 1-cm vertical incision is made with a scalpel entering the peritoneal cavity taking care not to injure underlying bowel or blood vessels. A finger is placed within this opening to ensure entrance into the intraperitoneal cavity. A suture is then placed into the fascia to secure the Hasson port and also for eventual closure. A 12 mm Hasson trocar is then secured in place.
If the patient is obese, a Veress needle is initially placed into the left upper quadrant. Intra-abdominal positioning of the needle can be confirmed by aspiration and a negative saline drop test. Pneumoperitoneum is then established by insufflating the abdomen to a pressure of 15 mmHg with carbon dioxide. A 5 mm port is then placed into the left upper quadrant.
A 30° laparoscopic camera is then introduced and all four quadrants of the abdomen are visually inspected. If the Veress needle is used for access in the left upper quadrant, an additional 12 mm trocar is inserted inferior to the umbilicus. This is the primary camera port during the case and also allows for passage of the endo-GIA linear stapler. Two 5 mm trocars are subsequently placed under direct visualization: one in the left lower quadrant lateral to the left rectus muscle and the other in the suprapubic position (Fig. 21.2). This is performed with attention not to injure the bladder or inferior epigastric vessels. The patient is then placed in the Trendelenburg position with the right side up to facilitate visualization of the appendix.
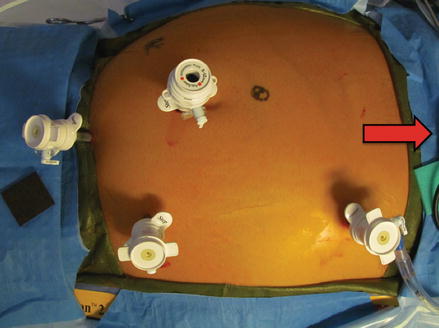
Figure 21.2
Trocar placement for laparoscopic appendectomy. One 12 mm trocar is placed below the umbilicus; one 5 mm trocar is placed in the left lower quadrant lateral to the rectus muscle; one 5 mm trocar is placed in the suprapubic position. One 5 mm trocar may be placed in the left upper quadrant if a Veress needle is used for access at this same point (optional). Red arrow marks the head of the patient
Identification of Appendix
The cecum and terminal ileum are mobilized away from the retroperitoneum with scissors or electrocautery allowing improved access to the base of the appendix and mesoappendix (Figs. 21.3 and 21.4). This step is critical in being able to identify the appendiceal base. The tip of the appendix is grasped and retracted medially and anteriorly providing complete exposure.
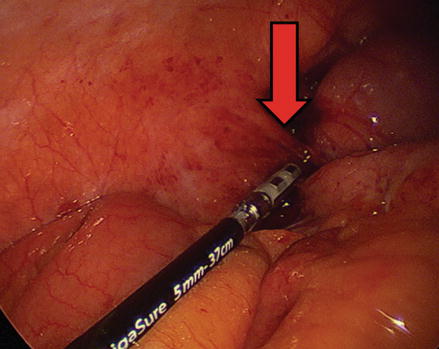
Figure 21.3




Retroperitoneal attachments of the cecum and terminal ileum. Access to the base of the appendix and mesoappendix may be difficult when there are robust retroperitoneal attachments between the cecum and the abdominal wall. Red arrow marks a retroperitoneal attachment
Related posts:






Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
