CHAPTER 97
Ankle Sprain
(Twisted Ankle)
Presentation
Patients usually describe stepping off a curb or into a hole. Sports-related injuries often occur after jumping and landing on another player’s foot, which causes an inversion or supination of the ankle. Of all ankle sprains, 85% are inversion injuries. The sensation of a “pop” or “snap” at the time of injury with immediate loss of function suggests disruption of a ligament. Severe swelling in the first hour suggests bleeding from the torn ends. The body’s response to the injury begins with inflammation, which produces swelling, warmth, pain, and stiffness that build to a maximum about 1 day after the injury.
Patients usually arrive either immediately after the injury or 1 to 2 days later, complaining of pain, swelling, and partial or complete inability to walk. Patients are usually tender around the lateral malleolus, particularly anteriorly, because the anterior talofibular ligament is the first to tear when the ankle is inverted. Although the pain during the first hours after injury is often localized to the injured area, it soon becomes diffuse during the first few days. After a few days, careful palpation will confirm which ligaments were most likely injured.
What To Do:
 Get a detailed description of the mechanism of injury, and ask if the patient could bear weight immediately after the injury. Ask if there have been previous injuries of the ankle. (Patients with a previous ankle injury have an increased risk for recurrence.)
Get a detailed description of the mechanism of injury, and ask if the patient could bear weight immediately after the injury. Ask if there have been previous injuries of the ankle. (Patients with a previous ankle injury have an increased risk for recurrence.)
 Document the degree and location of swelling and discoloration. Check the sensation and circulation distal to the injury. (A slight decrease relative to the uninjured foot might be attributed to the swelling.)
Document the degree and location of swelling and discoloration. Check the sensation and circulation distal to the injury. (A slight decrease relative to the uninjured foot might be attributed to the swelling.)
 Palpate sites of potential injury: the fibula up to the knee, the base of the fifth metatarsal on the lateral foot, the tarsal navicular bone anteriorly, the deltoid ligament medially, and, finally, the anterior talofibular ligament in front of the lateral malleolus. Note if there is tenderness along the posterior distal 6 cm of the lateral malleolus, the posterior medial malleolus, or the tip of either malleolus. Start palpating gently and away from the injury to overcome patients’ tendency to flinch at the first touch. Save the most likely site of injury for last, because the pain may inhibit any further examination.
Palpate sites of potential injury: the fibula up to the knee, the base of the fifth metatarsal on the lateral foot, the tarsal navicular bone anteriorly, the deltoid ligament medially, and, finally, the anterior talofibular ligament in front of the lateral malleolus. Note if there is tenderness along the posterior distal 6 cm of the lateral malleolus, the posterior medial malleolus, or the tip of either malleolus. Start palpating gently and away from the injury to overcome patients’ tendency to flinch at the first touch. Save the most likely site of injury for last, because the pain may inhibit any further examination.
 If there is not too much pain, check joint stability with the anterior drawer test (Figure 97-1) and the talar tilt test (Figure 97-2). Perform these tests gently. For the anterior drawer test, grasp the tibia with one hand and the heel with the other hand; with the ankle in slight plantar flexion, push the leg posterior while holding the foot still or pushing anteriorly. Anterior displacement of the talus can be felt or seen as a dimple over the anterolateral ankle compared with the uninjured side. A positive anterior drawer indicates a significantly torn anterior talofibular ligament. The talar tilt test is also performed with the foot in the neutral position. Gently invert the ankle and compare the range of movement and the mushiness of the end point with the uninjured side. An intact calcaneofibular ligament should prevent inversion. Often these tests cannot be accomplished because the ankle is too painful, in which case the tests may be deferred for up to 1 week.
If there is not too much pain, check joint stability with the anterior drawer test (Figure 97-1) and the talar tilt test (Figure 97-2). Perform these tests gently. For the anterior drawer test, grasp the tibia with one hand and the heel with the other hand; with the ankle in slight plantar flexion, push the leg posterior while holding the foot still or pushing anteriorly. Anterior displacement of the talus can be felt or seen as a dimple over the anterolateral ankle compared with the uninjured side. A positive anterior drawer indicates a significantly torn anterior talofibular ligament. The talar tilt test is also performed with the foot in the neutral position. Gently invert the ankle and compare the range of movement and the mushiness of the end point with the uninjured side. An intact calcaneofibular ligament should prevent inversion. Often these tests cannot be accomplished because the ankle is too painful, in which case the tests may be deferred for up to 1 week.
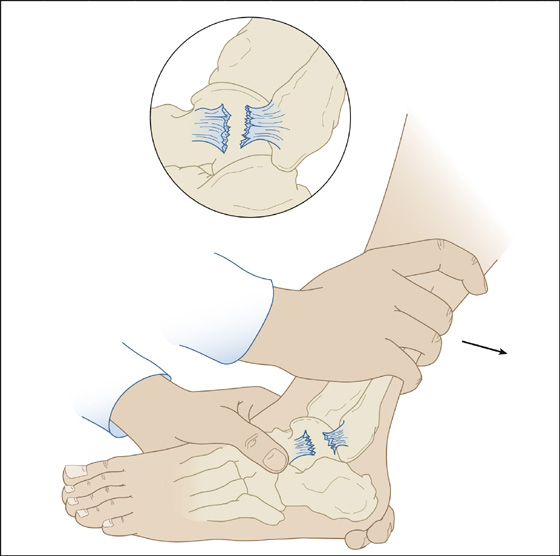
Figure 97-1 Anterior drawer test.

Figure 97-2 Talar tilt test.
 If there is significant medial ankle injury or severe lateral injury, perform a squeeze test to determine if there is a tear of the syndesmosis between the distal tibia and fibula. With the knee flexed at 90 degrees, place your hand over the midportion of the lower leg, with your thumb on the fibula and your fingers on the medial tibia. Squeeze the fibula and tibia together. Pain during this test signifies syndesmotic injury, predicts a prolonged recovery, and calls for an orthopedic referral. This may be associated with a fracture of the fibular head and is called a Maisonneuve fracture when there is an associated deltoid ligament tear or medial malleolus fracture.
If there is significant medial ankle injury or severe lateral injury, perform a squeeze test to determine if there is a tear of the syndesmosis between the distal tibia and fibula. With the knee flexed at 90 degrees, place your hand over the midportion of the lower leg, with your thumb on the fibula and your fingers on the medial tibia. Squeeze the fibula and tibia together. Pain during this test signifies syndesmotic injury, predicts a prolonged recovery, and calls for an orthopedic referral. This may be associated with a fracture of the fibular head and is called a Maisonneuve fracture when there is an associated deltoid ligament tear or medial malleolus fracture.
 Elevate the foot (preferably above the level of the heart), and for acute injuries apply an ice pack for 20 minutes and compress the ankle with a splint or elastic bandage.
Elevate the foot (preferably above the level of the heart), and for acute injuries apply an ice pack for 20 minutes and compress the ankle with a splint or elastic bandage.
 Optional radiographs of the ankle or foot may be ordered to rule out a fracture, but radiographs are not necessary (and likely to be negative) unless there was either (1) inability to bear weight both immediately and at the initial physical examination or (2) bony tenderness to palpation of the ankle in the posterior distal 6 cm of the lateral malleolus or the posterior distal medial malleolus, or bony tenderness of the foot at the tarsal navicular or the base of the fifth metatarsal bone. The use of these decision rules must remain secondary to the judgment and common sense of the clinician. Patient satisfaction can be maintained by informing patients, “Studies show that your type of ankle sprain does not need an x-ray, and I would prefer not to expose you to unnecessary irradiation.” You can still give the autonomy of decision making to the patient by stating, “I’d be glad to order an x-ray if you still want it.”
Optional radiographs of the ankle or foot may be ordered to rule out a fracture, but radiographs are not necessary (and likely to be negative) unless there was either (1) inability to bear weight both immediately and at the initial physical examination or (2) bony tenderness to palpation of the ankle in the posterior distal 6 cm of the lateral malleolus or the posterior distal medial malleolus, or bony tenderness of the foot at the tarsal navicular or the base of the fifth metatarsal bone. The use of these decision rules must remain secondary to the judgment and common sense of the clinician. Patient satisfaction can be maintained by informing patients, “Studies show that your type of ankle sprain does not need an x-ray, and I would prefer not to expose you to unnecessary irradiation.” You can still give the autonomy of decision making to the patient by stating, “I’d be glad to order an x-ray if you still want it.”
 Be liberal in imaging patients with other distracting painful injuries, altered sensorium, intoxication, paraplegia, or bone disease. Weight bearing is defined as the ability to transfer weight twice onto each leg for a total of four steps, regardless of limping. Assess ability to bear weight after determining bony tenderness, and do not coerce the patient.
Be liberal in imaging patients with other distracting painful injuries, altered sensorium, intoxication, paraplegia, or bone disease. Weight bearing is defined as the ability to transfer weight twice onto each leg for a total of four steps, regardless of limping. Assess ability to bear weight after determining bony tenderness, and do not coerce the patient.
 After the probability of a fracture has been ruled out, instruct the patient to elevate and rest the ankle as much as possible. When there is significant swelling, apply ice for three or four periods of 15 to 20 minutes a day for 3 days, insulating the skin from the ice with a compressive dressing to prevent frostbite and further reduce swelling. This, along with elevation, helps to minimize hemorrhage, inflammation, and pain.
After the probability of a fracture has been ruled out, instruct the patient to elevate and rest the ankle as much as possible. When there is significant swelling, apply ice for three or four periods of 15 to 20 minutes a day for 3 days, insulating the skin from the ice with a compressive dressing to prevent frostbite and further reduce swelling. This, along with elevation, helps to minimize hemorrhage, inflammation, and pain.
 Patients with mild to moderate sprains (grades I and II) should be fitted with a stirrup-type splint (Figure 97-3) that prevents inversion and eversion of the ankle, should be given crutches and instructions how to ambulate with crutches, and should be prescribed nonsteroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen, 200 to 800 mg q6h. (Add a proton-pump inhibitor, such as omeprazole [Prilosec], or a high dose of an H2-receptor antagonist, such as ranitidine [Zantac], to reduce NSAID-related dyspepsia.) Acetaminophen (Tylenol) may be just as effective as NSAIDs for pain relief and completely avoids the potential for gastrointestinal (GI) side effects. Narcotic analgesics may be required (especially at night) for the first few days. For follow-up, instruct the patient to begin weight bearing using a stirrup splint as soon as it is tolerable, then for the next 4 to 6 weeks, and to use crutches for the shortest time possible. Once normal weight bearing and pain-free range of motion are achieved, muscle strengthening can begin. Early phases of treatment should begin with low resistance, such as stationary cycling or swimming. Further strengthening can be accomplished using eversion exercises, which should be performed in dorsiflexion to strengthen the peroneus brevis and tertius, and in plantar flexion to strengthen the peroneus longus. These sprains can be referred to a primary care specialist for follow-up in 2 weeks.
Patients with mild to moderate sprains (grades I and II) should be fitted with a stirrup-type splint (Figure 97-3) that prevents inversion and eversion of the ankle, should be given crutches and instructions how to ambulate with crutches, and should be prescribed nonsteroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen, 200 to 800 mg q6h. (Add a proton-pump inhibitor, such as omeprazole [Prilosec], or a high dose of an H2-receptor antagonist, such as ranitidine [Zantac], to reduce NSAID-related dyspepsia.) Acetaminophen (Tylenol) may be just as effective as NSAIDs for pain relief and completely avoids the potential for gastrointestinal (GI) side effects. Narcotic analgesics may be required (especially at night) for the first few days. For follow-up, instruct the patient to begin weight bearing using a stirrup splint as soon as it is tolerable, then for the next 4 to 6 weeks, and to use crutches for the shortest time possible. Once normal weight bearing and pain-free range of motion are achieved, muscle strengthening can begin. Early phases of treatment should begin with low resistance, such as stationary cycling or swimming. Further strengthening can be accomplished using eversion exercises, which should be performed in dorsiflexion to strengthen the peroneus brevis and tertius, and in plantar flexion to strengthen the peroneus longus. These sprains can be referred to a primary care specialist for follow-up in 2 weeks.

Figure 97-3 Grade I and II sprains should be fitted with a stirrup splint.
 Patients with moderate to severe sprains (grades II and III) should be placed in a soft, bulky compression dressing. If there is instability or fracture, incorporate a plaster/fiberglass sugar-tong splint (Figure 97-4) that extends almost the entire length of the tibia and fibula just below the knee. Alternatively, when available, a fracture boot or short-leg walking cast can be used with full weight bearing for the first 5 to 7 days (Figure 97-5). This allows the patient to eliminate the need for crutches and makes activities of daily living much easier. Recovery and rehabilitation can proceed as described for grade I and II sprains. Narcotic analgesics like hydrocodone will likely be needed for pain relief along with NSAIDs or acetaminophen.
Patients with moderate to severe sprains (grades II and III) should be placed in a soft, bulky compression dressing. If there is instability or fracture, incorporate a plaster/fiberglass sugar-tong splint (Figure 97-4) that extends almost the entire length of the tibia and fibula just below the knee. Alternatively, when available, a fracture boot or short-leg walking cast can be used with full weight bearing for the first 5 to 7 days (Figure 97-5). This allows the patient to eliminate the need for crutches and makes activities of daily living much easier. Recovery and rehabilitation can proceed as described for grade I and II sprains. Narcotic analgesics like hydrocodone will likely be needed for pain relief along with NSAIDs or acetaminophen.
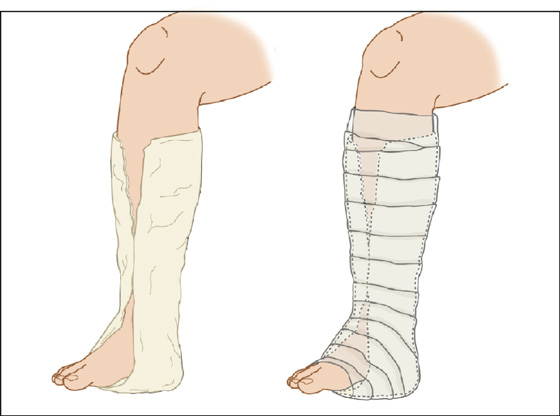
Figure 97-4 Severe sprains and fractures should be treated with a “sugar-tong” splint or Jones dressing.
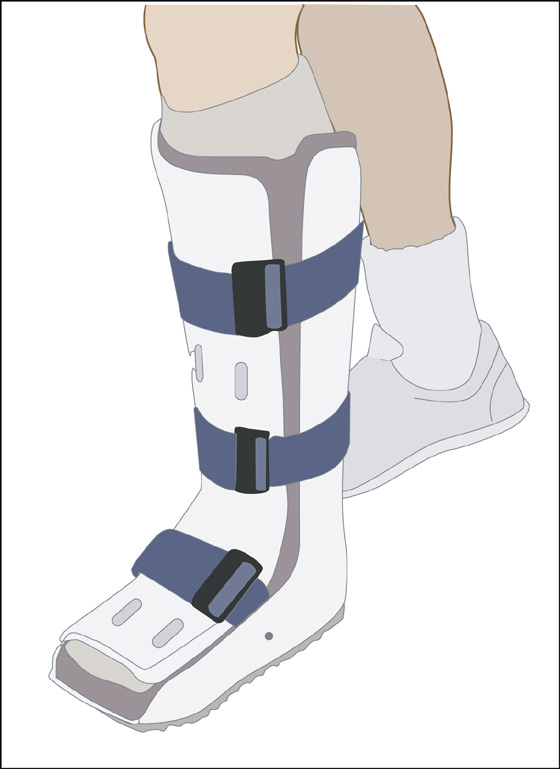
Figure 97-5 Walking boot for grade III sprains.
 Moderate to severe sprains, recurrent sprains, sprains with instability or syndesmotic injury, and most injuries with associated fractures should be seen by an orthopedic surgeon within 1 week. Obtain orthopedic consultation in cases of delayed recovery, diagnostic uncertainty, neurovascular compromise, pain out of proportion to the injury (think compartment syndrome), and treatment involving competitive athletes.
Moderate to severe sprains, recurrent sprains, sprains with instability or syndesmotic injury, and most injuries with associated fractures should be seen by an orthopedic surgeon within 1 week. Obtain orthopedic consultation in cases of delayed recovery, diagnostic uncertainty, neurovascular compromise, pain out of proportion to the injury (think compartment syndrome), and treatment involving competitive athletes.
 Tender or swollen ankle sprains in children with open growth plates are considered to be nondisplaced physeal (Salter I) fractures, even with negative radiographs, and are usually immobilized for 3 to 4 weeks. Bony structures and growth plates are often weaker than the contiguous ligaments and tendons. Care should be taken to palpate both malleoli and their respective physes, the proximal fifth metatarsal (a site of peroneus brevis avulsion), and the tarsal navicular, which may reveal an occult fracture.
Tender or swollen ankle sprains in children with open growth plates are considered to be nondisplaced physeal (Salter I) fractures, even with negative radiographs, and are usually immobilized for 3 to 4 weeks. Bony structures and growth plates are often weaker than the contiguous ligaments and tendons. Care should be taken to palpate both malleoli and their respective physes, the proximal fifth metatarsal (a site of peroneus brevis avulsion), and the tarsal navicular, which may reveal an occult fracture.
 Patients not receiving radiographs at the initial visit should be instructed to seek follow-up if their symptoms have not improved after 1 week. Persistent ankle pain beyond 6 to 8 weeks could indicate a complication or overlooked injury. MRI, which is seldom needed at the initial presentation, may be very useful if symptoms have persisted this long.
Patients not receiving radiographs at the initial visit should be instructed to seek follow-up if their symptoms have not improved after 1 week. Persistent ankle pain beyond 6 to 8 weeks could indicate a complication or overlooked injury. MRI, which is seldom needed at the initial presentation, may be very useful if symptoms have persisted this long.
What Not To Do:
 Do not have the patient apply heat during the recovery phase. It is unnecessary and increases the swelling.
Do not have the patient apply heat during the recovery phase. It is unnecessary and increases the swelling.
 Do not recommend ointments or creams. They offer no benefit for ankle sprains.
Do not recommend ointments or creams. They offer no benefit for ankle sprains.
 Do not overlook fractures of the anterior process of the calcaneus, the tarsal navicular, the talar dome or the rest of the talus, or the os trigonum, all visible on the ankle radiographs.
Do not overlook fractures of the anterior process of the calcaneus, the tarsal navicular, the talar dome or the rest of the talus, or the os trigonum, all visible on the ankle radiographs.
 Do not completely rule out a fracture based on a negative radiograph.
Do not completely rule out a fracture based on a negative radiograph.
Discussion
Blunt ankle trauma is one of the most common injuries seen in emergency departments, and ankle sprains are the most common sports-related orthopedic injury, but less than 15% have associated clinically significant fractures. The old tradition of radiographic examination of all ankle injuries is no longer required, and the Ottawa decision rules described here have led to reductions in the number of negative radiographs, use of unnecessary radiation, and waiting times and costs, all without missed fractures or patient dissatisfaction.
The ankle ligaments can be divided into three groups: lateral ligaments, medial ligaments, and the ligaments of the syndesmosis. The most common injuries involve the lateral ligaments. These three groups of ligaments function as the static stabilizers of the ankle joint. The dynamic stabilizers consist of the muscles of the anterior, lateral, and posterior compartments of the leg. Mild or grade I sprains usually involve partial tearing of ligament fibers and minimal swelling, with no joint instability. Moderate or grade II sprains are characterized by some pain, edema, ecchymosis, and point tenderness over the involved structures, resulting in partial loss of joint motion. Some ligament fibers may be completely torn, but overall stability of the joint remains intact. Severe or grade III sprains exhibit gross instability with complete tearing of all ligament fibers, marked swelling, and severe pain. In general, the more extensive the ligament injury, the more difficult it is to bear weight, the more swelling noted acutely, and the more ecchymosis that develops over a few days.
Medial ligament injuries usually result from an eversion stress. Because the deltoid ligament is so strong, it is rarely injured in isolation but rather in association with lateral malleolus fracture.
Current research recommends the combination of early weight bearing and immobilization for lateral ligament injuries. Four stages characterize the biology behind functional treatment of acute lateral ankle ligament tears. Immediately after the injury, hemorrhage, swelling, inflammation, and pain are best treated with rest, ice, compression, and elevation (RICE). During the following 1 to 3 weeks, called the healing or proliferation phase, fibroblasts invade the injured area and proliferate to form collagen fibers. Protection in the form of a brace should be used during this time. Stirrup-style braces provide the best support. Three weeks after the injury, the maturation phase begins, during which the collagen fibers mature and become scar tissue. Controlled stretching of muscles and movement of the joint encourage the orientation of the collagen fibers along the stress lines, creating a stronger ligamentous repair. After 6 to 8 weeks, the new collagen fibers can withstand almost normal stress, and full return to activity is the goal. The entire maturation and remodeling of the injured ligaments lasts from 6 to 12 months. Reports indicate that up to 73% of people who sustain a lateral ankle sprain have recurrent sprains, but it is unknown how many of these participants partake in rehabilitation.
A minor sprain usually keeps an athlete out of competition for several days to 2 weeks, and a moderate sprain usually keeps an athlete out of competition for 2 to 4 weeks. Time to return to play for severe sprains will be greater than 4 weeks. Taping, lace-up braces, and air stirrup orthoses can all be helpful in the rehabilitation of ankle injuries.
When the patient reports a snapping sensation and states that it felt like something “slipped out of place,” accompanied by pain in the posterolateral aspect of the ankle, consider the diagnosis of a peroneal tendon dislocation. This is seen more frequently in skiers but does occur to a lesser extent in other sport activities. Swelling and tenderness is found posteriorly and extending 6 inches proximally from the lateral malleolus. Circumduction of the ankle with palpation over the peroneal tendons may elicit a dislocation or subluxation of the peroneal tendons. These injuries require orthopedic consultation and may require acute surgical repair to prevent recurrence.
Typically, a patient with a Maisonneuve fracture will not complain of pain in the region of the proximal fibula but rather only of ankle pain in the region of the medial malleolus. Morbidity associated with proximal fibular fractures includes contusion or laceration of the common peroneal nerve (resulting in footdrop), injury to the anterior tibial artery, damage to the lateral collateral ligament of the knee, and even compartment syndrome.
The application of ice (cryotherapy) for the prevention of swelling and inflammation is generally accepted as a standard of care for the treatment of sprains. Although it is theorized that cryotherapy can be beneficial both immediately after injury and in the rehabilitation phase, the available scientific evidence does not provide much support for this belief. Therefore it is still not possible to make confident recommendations to our patients concerning the optimal type, frequency, timing, and duration of ice application. It is certainly reasonable to downplay its importance and see that a patient does not suffer further discomfort by applying such cold packs. Compression and elevation will be most effective in reducing the swelling after an ankle sprain.
A Thompson test should be performed if inspection and examination of the Achilles tendon suggests a full or partial tear there (see Figure 126-1).
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


