CHAPTER 31 Ankle block
Clinical anatomy
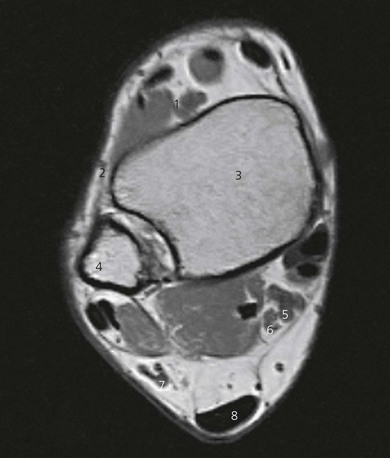
The tibial nerve runs deep to the flexor retinaculum and posterior to the posterior tibial vein and artery, between the Achilles’ tendon and medial malleolus (Figs 31.1 and 31.2). It divides into medial and lateral plantar nerves providing sensory innervation to the medial side of the sole of the foot and heel. The tibial nerve provides motor supply to the intrinsic muscles of the foot. It is the largest nerve at the ankle, requiring the longest block onset, and thus should be blocked first.

The superficial peroneal nerve travels distally with the peroneus brevis muscle, becoming superficial above the lateral malleolus, and runs over the dorsum of the foot, to which it provides sensory innervation (Figs 31.2 and 31.3).

The sural nerve runs superficially with the small saphenous vein and lies subcutaneously between the lateral malleolus and Achilles, tendon (Figs 31.2 and 31.4). It provides sensory innervation to the lateral aspect of the ankle and foot.

Surface anatomy
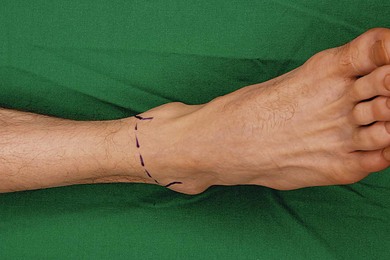
Important bony structures for the ankle block include the medial and lateral malleoli and the calcaneum. Other landmarks include the Achilles’ tendon, and on the ventral aspect of the ankle, the anterior tibial artery pulse and extensor hallucis longus tendon (Fig. 31.5). These tendons can be accentuated if the patient dorsiflexes the foot against resistance. A single needle insertion site at the midpoint of the intermalleolar line on the ventral aspect of the ankle is used for block of the superficial and deep peroneal nerves and saphenous nerve. Needle insertion for sural and tibial block is adjacent to the Achilles tendon, at the level of the superior aspect of the medial and lateral malleoli, respectively.
Sonoanatomy
Tibial nerve
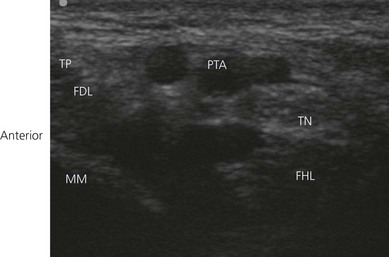
Position the patient supine and bolster the foot with a pillow to expose the anterior and medial portion of the lower leg and foot. The lower limb is externally rotated. Place a 10–15 MHz transducer immediately above the medial malleolus to locate the tibial nerve in the transverse (short axis) view (Fig. 31.6). Perform a systematic anatomical survey in the medial aspect of the ankle. The bony medial malleolus is easily identified (bony shadow). Move the transducer slightly posteriorly to identify the tibialis posterior and flexor digitorum longus tendons. Both tendons are found within the flexor retinaculum of the ankle. They display a sliding movement with ankle flexion and are often hyperechoic. Then identify the pulsatile posterior tibial artery (Doppler use is optional). The tibial nerve at the ankle is often round to oval with a honeycomb appearance (Fig. 31.7). It is expected to lie posterior to the posterior tibial artery. Trace the tibial nerve proximally. The nerve is larger and is easier to identify more cephalad in the leg. It is also easy to image the nerve longitudinally by rotating the transducer 90°.

Deep peroneal nerve
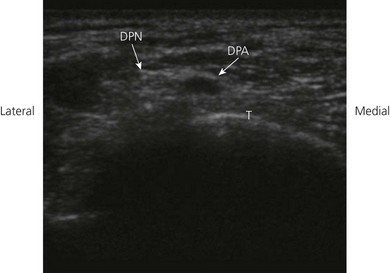
Position the patient supine and bolster the foot with a pillow to expose the anterior and medial portion of the lower leg and foot. The lower limb is in the neutral position. The small deep peroneal nerve may be difficult to locate. This nerve lies adjacent to the anterior tibial vessels (above the ankle) and the dorsalis pedis at the ankle region. A 10–15 MHz transducer is placed on the dorsum of the foot along the intermalleolar line to locate the dorsalis pedis artery in the transverse view (Fig. 31.8) The predominantly hypoechoic deep peroneal nerve is found lateral to the dorsalis pedis artery and the extensor hallucis longus tendon (Fig. 31.9).

< div class='tao-gold-member'>






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


