CHAPTER 32 Anesthesia for Pediatric Dentistry
In light of the advances in health care, dental disease is still among the most prevalent of diseases, according to the Centers for Disease Control and Prevention (CDC). Although dental caries (tooth decay) is largely preventable, it remains the most common chronic disease of children aged 6 to 11 years, and of adolescents aged 12 to 19 years. Tooth decay is more common than many other common chronic diseases of childhood including asthma. It is four times more common than asthma among adolescents aged 14 to 17 years (CDC Division of Oral Health). Maternal nutritional and behavioral influences are very strong factors that propagate transmission of caries from the mother to her infant (American Academy of Pediatrics, 2003). The impact of caries is pervasive; poor nutrition may cause them or be the result of them. However, fluoridation of community water supplies, use of children’s vitamins containing fluoride, and increased awareness of dental hygiene have produced a significant reduction in dental caries in the general population.
Despite advances in preventive dentistry, some conditions still require more than local anesthesia to facilitate dental treatment. General anesthesia may be required to treat children with severe systemic disease or disabling congenital anomalies, as well as infants and toddlers with milk-bottle caries who require partial or complete oral rehabilitation. General anesthesia may also be required for children and adolescents with severe developmental delay who require a safe and effective environment to render the necessary dental treatment. In addition, the fearful or combative child may require procedural sedation when behavior modification techniques have not succeeded. Proper care for these populations necessitates a care team approach, consisting of properly trained anesthesia and dental providers. A glossary of commonly used dental terms is shown in Table 32-1.
TABLE 32-1 Glossary of Common Dental Terms
| Proper Name | Common Name or Definition |
| Abutment | Tooth or teeth on either side of an edentulous area supporting a bridge |
| Amalgam | Silver-coated restoration |
| Bicuspid | Premolar tooth (older term) |
| Bitewing | Dental radiograph that views several adjacent maxillary and mandibular teeth simultaneously; especially useful in evaluating dental caries |
| Bruxism | Involuntary tooth grinding |
| Burr | Drill bit used to prepare a tooth for caries restoration |
| Caries | Dental cavity or cavities |
| Composite | Tooth-colored restoration |
| Crown | Portion of the tooth seen in the mouth above the gum line; also, term used for the dental restoration of the same anatomic region; popularly known as a cap |
| Cuspid | Canine tooth (older term) |
| Diastemata | Separations between the teeth; commonly seen between the maxillary central incisors |
| Dry socket | Nonhealing extraction site |
| Endodontic therapy | Root canal therapy |
| Exfoliation | Spontaneous loss of a tooth |
| Exodontia | Dental extraction |
| Eye tooth | Canine tooth (familiar term) |
| Gingivitis | Inflammation of superficial aspects of the peridontium |
| Handpiece | Dental drill |
| Ludwig’s angina | Dental infection of the floor of the mouth involving the submandibular, submaxillary, and submental spaces bilaterally |
| Milk tooth | Primary or baby tooth |
| Occlusion | Patient’s “bite” |
| Oral prophylaxis | Dental cleaning |
| Overbite | Degree of vertical overlap of the maxillary teeth over the mandibular teeth |
| Overjet | Degree of horizontal projection of the maxillary teeth beyond the mandibular teeth |
| Periapical | Area surrounding the apex of the root; a periapical dental radiograph also includes the clinical crown of the tooth |
| Periodontium | Soft and hard tissues surrounding and supporting teeth |
| Pulpotomy | Therapeutic removal of the coronal portion of the dental pulp |
| Pyorrhea | Common name for periodontal inflammation, or gum disease; except for gingivitis, periodontal disease is rare in children |
| Rubber dam | Square latex or vinyl sheet used to isolate the teeth from the oral cavity during dental treatments |
Human dentition
Dental Development
Initial calcification of the primary tooth buds may be seen in the fourth month of prenatal life. In general, by the end of the sixth prenatal month, all of the primary teeth have begun to develop. The newborn infant is edentulous, with the rare exception of a mandibular central incisor. This natal or neonatal tooth tends to be quite mobile, and in the past it was thought to require immediate extraction. Recent data suggest that by the end of the neonatal period, this mobile tooth becomes quite stable and capable of normal masticatory function. This is indeed fortunate for the infant, because these neonatal teeth are frequently the only primary teeth that develop in that position (King and Lee, 1989; Cunha et al., 2001).
The sequence of eruption of human teeth may critically affect infant feeding, behavioral, and masticatory skills. Major changes in the appearance of the dentition in the oral cavity probably alter important aspects of neurobehavioral development (Wright, 2000). As an example of eruption sequence alterations, premature infants and neonates requiring prolonged orotracheal intubation have significant defects in both oral and dental structures that may persist past age 5 years, even after removal of the orotracheal tube (Fadavi et al., 1992).
The order of appearance of the teeth in the oral cavity tends to follow generalized patterns (Table 32-2). Usually the teeth erupt in pairs. A mandibular right central incisor erupts at approximately the same time as the mandibular left central incisor, at approximately 6 to 7 months of age. The mandibular teeth usually precede their maxillary counterparts; the maxillary incisors erupt approximately 1 month later than the mandibular incisors. The eruption sequence continues and is usually complete by age 2 to 2½ years. The last tooth to erupt is the deciduous second molar, called the 2-year molar because of its appearance at age 2 years.
TABLE 32–2 Eruption Sequence of the Human Dentition
| Approximate Age Eruption Begins | Approximate Age Eruption Is Completed | |
| Primary Dentition | ||
| Maxillary | ||
| Central incisor | 7½ mo | 1½ yr |
| Lateral incisor | 9 mo | 2 yr |
| Cuspid | 18 mo | 3¼ yr |
| First molar | 14 mo | 2½ yr |
| Second molar | 24 mo | 3 yr |
| Mandibular | ||
| Central incisor | 6 mo | 1½ yr |
| Lateral incisor | 7 mo | 1½ yr |
| Cuspid | 16 mo | 3¼ yr |
| First molar | 12 mo | 2¼ yr |
| Second molar | 20 mo | 3 yr |
| Permanent Dentition | ||
| Maxillary | ||
| Central incisor | 7–8 yr | 10 yr |
| Lateral incisor | 8–9 yr | 11 yr |
| Cuspid | 11–12 yr | 13–15 yr |
| First bicuspid | 10–11 yr | 12–13 yr |
| Second bicuspid | 10–12 yr | 12–14 yr |
| First molar | 6–7 yr | 9–10 yr |
| Second molar | 12–13 yr | 14–16 yr |
| Mandibular | ||
| Central incisor | 6–7 yr | 9 yr |
| Lateral incisor | 7–8 yr | 10 yr |
| Cuspid | 9–10 yr | 12–14 yr |
| First bicuspid | 10–12 yr | 12–13 yr |
| Second bicuspid | 11–12 yr | 13–14 yr |
| First molar | 6–7 yr | 9–10 yr |
| Second molar | 11–13 yr | 14–15 yr |
From Schour I, Massler M: The development of the human dentition, JADA 28:1153, 1941. Reprinted by permission of ADA Publishing.
When completed, the primary dentition totals 20 teeth (Wright, 2000). As the toddler’s growth continues, the mandible and maxilla enlarge, causing separations, also known as diastemata, between the primary teeth (Zwemer, 1993). The diastemata increase as the primary teeth are beginning to exfoliate and the permanent or succedaneous teeth begin to erupt. The separations also permit sufficient room for the proper alignment of the permanent dentition.
The maintenance of the health and hygiene of the primary teeth is essential to avoid premature tooth loss. When primary teeth are prematurely lost as a result of decay or trauma, the space needed for the permanent tooth eruption is also lost because the natural tendency of the tooth is to tip mesially (toward the midline) in the oral cavity. Subsequently, dental malocclusions tend to occur. Finally, the primary teeth may also function as the permanent teeth if the permanent analogous tooth fails to develop (Wright, 2000).
Development of the secondary, or permanent, dentition begins at birth with calcification of the buds of the permanent first molars. The permanent dentition begins its eruption pattern with the permanent first molar, usually at approximately 6 years of age. Like their primary counterparts, the mandibular teeth usually precede the maxillary teeth, with the permanent mandibular incisors beginning to appear at approximately age 6 to 7 years. Unlike the primary dentition, where there is usually a variability of several months in the timing of eruption, the permanent teeth may vary as much as 1 to 2 years in eruption sequence. After eruption of the permanent first molars, eruption of the remaining permanent teeth then occurs in this sequence: mandibular central incisors, maxillary central incisors, mandibular lateral incisors, maxillary lateral incisors, mandibular cuspids, maxillary and mandibular first premolars, maxillary and mandibular second premolars, maxillary cuspids, and mandibular and maxillary second molars (see Table 32-2). At the completion of the eruption sequence, the permanent dentition consists of 32 teeth (Wright, 2000).
In addition to the frequently absent third molars, two other permanent tooth forms are sometimes congenitally absent. The mandibular premolars and the maxillary lateral incisors may be congenitally absent, either singly or in symmetric pairs (Neville et al., 2002). Occasionally, a tooth that is thought to be congenitally absent is actually impacted in the soft tissues or alveolar bone.
Just as there are congenitally absent teeth, there are supernumerary or accessory teeth. The most common supernumerary tooth is the mesiodens, a conically shaped tooth consistently located in the midline between the maxillary central incisors. Other supernumerary teeth are the third premolars and fourth maxillary molars (Neville et al., 2002).
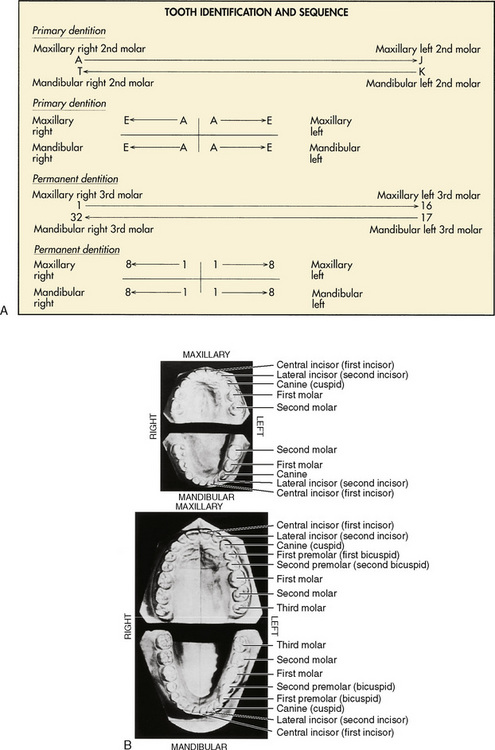
Dental Identification
There are two principal universal dental identification systems. In both systems, the primary teeth are designated by letters, and the permanent teeth are designated by numbers. These systems differ in the way that the dental arches (mandible and maxilla) are divided. The first system uses a sequential means for identification, with the primary maxillary right second molar designated as tooth A and followed sequentially around the contralateral side of the maxilla to the left second molar, which is tooth J. The primary mandibular left second molar is tooth K, and the sequence is completed on reaching the mandibular right second molar, tooth T. Similarly, the numbering system for the permanent dentition starts with the maxillary right third molar as tooth 1 and continues to the maxillary left third molar, tooth 16. The sequence continues with the mandibular left third molar, tooth 17, and is completed with the mandibular right third molar, tooth 32 (Herlich, 1990). Both pediatric and general dentists commonly use this system of tooth identification.
The second designation system divides the dental arch into quadrants. All primary central incisors are tooth A and follow distally or posteriorly, so that all primary second molars are tooth E. To make the designation more specific, the quadrant is also named. For example, the primary maxillary right lateral incisor is designated maxillary right B. Similarly, the permanent dentition is divided into quadrants. All central incisors are tooth 1 and continue posteriorly, so that all third molars are tooth 8. This system is most commonly used by orthodontists (Fig. 32-1).
Dental Anatomy and Physiology
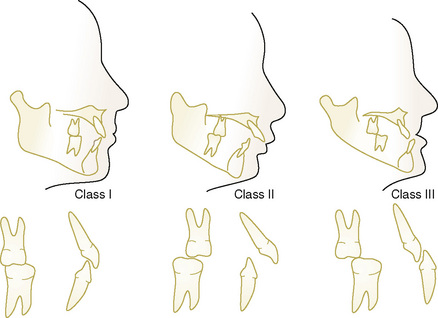
The tooth is composed of a crown, which is usually visible for clinical examination, and a root, which is not seen during routine clinical examination. They are separated by the cementoenamel junction or cervical region of the tooth (Fig. 32-2). The cementoenamel junctions are seen more commonly in adult dentition if gingival (“gum”) recession occurs. The crown is responsible for the slicing, ripping, and grinding of foodstuffs (incisors, canines, and molars, respectively). The root structure imparts stability to the tooth in its surrounding tissues. The anterior teeth, the incisors and the canines, are single rooted with a conical shape. The posterior teeth, the premolars and molars, are multirooted and impart most of their stability by both the number of roots and the subtly divergent directions in which the roots may grow.
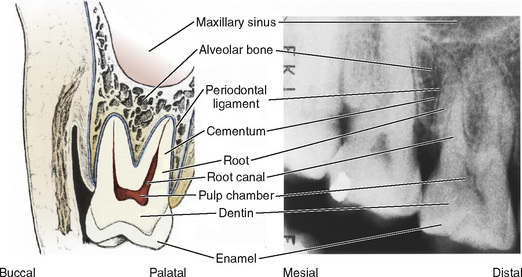
FIGURE 32-2 Schematic (left) and radiographic (right) views of a right maxillary molar.
(Modified with permission from Ash MM Jr, editor: Wheeler’s dental anatomy, physiology, and occlusion, ed 7, Philadelphia, 1993, Saunders, p 6.)
The individual teeth are composed of enamel, dentin, dental pulp, and cementum (Wright, 2000) (see Fig. 32-2). The enamel covers the external surface of the dental crown. It is the hardest substance in the human body and, unlike bone, has no living cells. When intact, enamel functions as a thermal insulator and an impervious barrier to chemicals and microorganisms.
Another difference between the sets of dentition rests in the color of the enamel. The primary teeth are milky white, or opalescent; hence, the name milk teeth. The permanent teeth, on the other hand, are significantly less “milky” because pigment absorption has occurred during their development or has been acquired during the intraoral lifetime of the tooth (Wright, 2000). Two examples are tetracycline staining (developmental) and caffeine staining (acquired).
The pulp chambers of the primary teeth are larger than the permanent teeth because of the relative thinness of the deciduous enamel and dentin (Wright, 2000). Less than meticulous dental restorations or large carious lesions may predispose the primary teeth to pulpal or endodontic therapy earlier than their permanent counterparts.
The root structures of the primary molars are more saber shaped and extend laterally beyond the crown width. This unique root structure allows adequate room for the permanent tooth bud to develop and mature until the exfoliative process is completed for the primary tooth (Wright, 2000).
Dental pathophysiology
Orthodontic Pathology
Malocclusion is the improper alignment of the teeth and jaws or bad bite. A skeletal malocclusion describes a malalignment between the jaws. A dental malocclusion describes the interarch relationship between the upper and lower teeth. A malocclusion may be caused by both hereditary and environmental factors. Crowding, spacing, supernumerary teeth, hypodontia, and asymmetric jaw growth are determined mostly by inheritance. Environmental factors such as thumb sucking, dental caries, premature loss of primary teeth, and trauma also can contribute to malocclusion (Mossey, 1999). An untreated malocclusion can lead to tooth decay, periodontal disease, abnormal wear of teeth, difficulty in chewing and speaking, and poor self-image.
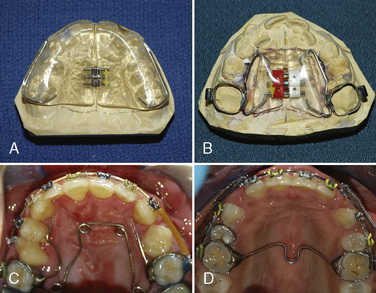
Edward H. Angle, who is regarded as the father of orthodontics, developed a classification system for malocclusion based on the sagittal (anteroposterior) relationship of the teeth and jaws (Angle, 1899). Angle believed the upper first molars were critical to occlusion, and that the upper and lower molars should meet so that the mesiobuccal cusp of the upper molar contacts in the buccal groove of the lower molar. If this molar relationship existed and the teeth were arranged on a smoothly curving line of occlusion, then normal occlusion would result (Fig. 32-3). Angle’s classification system is as follows:
Whether orthodontic treatment should occur in one or two phases of treatment is a source of controversy. Phase I, or early orthodontic treatment, may correct a problem when the patient still has primary teeth or has a combination of primary and permanent teeth. Some practitioners believe it may keep more serious problems from developing, and it may make treatment at a later age shorter or less complicated. Typically, early treatment involves the use of materials and techniques to guide or modify growth as adult teeth are erupting (Kluemper et al., 2000)
Appliances used in early treatment may be removable or fixed (cemented). They may be made of metal, ceramic, or acrylic. Examples of appliances used to address transverse discrepancies include palatal expanders, quad helixes, and transpalatal arches (Fig. 32-4). Headgear therapy may be used to treat anteroposterior discrepancies (class II or class III malocclusions) and are composed of a removable and fixed component. A lower lingual holding arch is a banded appliance used to maintain space for the eruption of permanent teeth in the mandibular arch (Fig. 32-5). Functional appliances change the position of the lower jaw to produce movement of teeth and modification of growth. Examples of functional appliances include the Twin block, Herbst appliance (Fig. 32-6), and Bionator.

Phase II or active treatment involves placement of fixed appliances (braces) or Invisalign in the permanent dentition (Boyd, 2008). Treatment times vary with several factors, including the severity of the problem being corrected, patient response to treatment, and patient compliance. Temporary anchorage devices (Fig. 32-7) are implants used to provide absolute anchorage and help move teeth (Cope, 2005). Patients use retainers to keep teeth in their new positions after treatment.

Combined surgical orthodontic treatment is used to treat patients with severe malocclusions or craniofacial anomalies. Presurgical orthodontic treatment is used to prepare patients for surgery by removing dental compensations and upright teeth over basal bone (Proffit and Miguel, 1995). In a traditional orthognathic procedure, a surgical splint may be fabricated and wired to the patient’s teeth. This splint may help the surgeon determine the final position of the jaws.
Nasoalveolar molding (NAM) is a presurgical orthopedic technique used to reduce the severity of the cleft deformity in infant patients with complete unilateral or bilateral cleft lip and palate (Grayson et al., 1999). The appliance is composed of a removable acrylic plate fabricated from an intraoral impression, and a nasal stent (Fig. 32-8). The amount of acrylic is sequentially reduced to decrease the separation between the greater and lesser alveolar segments. Once the gap between the alveolar segments is 5 mm or less, the nasal stent is added to mold the nasal cartilage. Lip or nasal repair occurs at 4 to 6 months of age. Patients with NAM can present for cleft lip surgery or ear, nose, and throat procedures such as myringotomy and tubes. The NAM appliance can be left in place during inhalation induction and mask ventilation, or it can be removed before the beginning of induction. The device should be removed before airway instrumentation for a laryngeal mask airway (LMA) or endotracheal tube.

Patient spectrum
The physically handicapped patient most likely to appear for pedodontal treatment has athetoid cerebral palsy, postencephalitis syndrome, profound mental retardation, or autistic behavior (Dougherty et al., 2001; Shenkin et al., 2001; Waldman and Perlman, 2001). For example, patients with cerebral palsy may be wheelchair bound and have significant difficulty in controlling athetoid motion. The use of nitrous oxide, which depresses involuntary movement, may ensure a higher success rate in dental treatments for patients with cerebral palsy (Kaufman et al., 1991). The pedodontist is specially trained to deal with these problems in the kindest and most expedient methods available regardless of the clinical setting (Rosenstein, 1978; Pope and Curzon, 1991).
The pediatric dentist is routinely called on to treat the medically compromised child or adolescent when the general practitioner is reluctant to get involved in treatment. For example, the pediatric dentist primarily treats the child with congenital heart disease, the insulin-dependent diabetic, the patient with craniofacial anomalies, or the child with oncologic diseases in conjunction with the pediatrician or primary care physician. Both fear and lack of training may cause the general dentist to feel quite uncomfortable in treating the compromised child or adolescent. In addition, the general dental practitioner frequently lacks the physical resources, such as specialized equipment, to care for these patients. The pediatric dentist is usually quite comfortable in recommending and prescribing antibiotic prophylaxis for subacute bacterial endocarditis (SBE), for example, and keeps current with appropriate timing in dosage, effectiveness, and relative risks (Wahl, 1994; Hayes and Fasules, 2001; American Academy of Pediatric Dentistry, 2002e).
Dentist’s needs and techniques
The pediatric dental patient requiring anesthesiology services usually needs many dental procedures during a single anesthetic administration. The quality of dental restorations is probably improved under general anesthesia (Tate et al., 2002; Al-Eheideb and Herman, 2003). In addition, the parents of children who have had general anesthesia for pediatric dental care have greater satisfaction than parents of children who did not have general anesthesia (Acs et al., 2001). After induction of general anesthesia and protection of the airway, the anesthesiologist, the anesthesia machine, and the anesthesia equipment cart are positioned at either the patient’s head or side.
The dentist’s first step is to obtain necessary intraoral radiographs of the teeth (periapical, bitewing, and occlusal radiographs). The dentist then performs a clinical examination. After placement of a pharyngeal pack (which should be noted on the anesthesia record), dental impressions may be taken if future orthodontic treatment is anticipated. Also, the dentist usually places a rubber dam around the dental arch to be treated. Despite its name, the rubber dam is not usually latex. Nevertheless, if the patient is latex sensitive, care must be taken to ensure that nonlatex products are being used. The rubber dam is held in place by a metal clamp that grasps the dental crown. A substantial length of dental floss or umbilical tape is tied around the clamp before its placement, to prevent inadvertent loss in the aerodigestive tract. Except for extractions and oral prophylaxis, the remainder of the treatment is performed with the rubber dam in place. Caries removal and tooth restoration take place with silver amalgam, tooth-colored composite, or preformed crowns. The rubber dam affords the dentist a dry environment in which the dental materials can cure optimally and achieve their greatest compressive and tensile strength. The rubber dam is also a barrier to protect the patient from iatrogenic dental trauma, including the accidental loss of dental materials or broken instruments and their possible entrance into the aerodigestive tract. The application of topical fluorides takes place after all of the restorative dentistry is completed with the rubber dam still in place (Mathewson and Primosch, 1995).
Pediatric dentistry may also encompass the need for oral and maxillofacial surgery. Oral and maxillofacial surgeons frequently perform these procedures after extensive training. Many oral and maxillofacial surgeons have dual dental and medical training, as well as fellowship training in head and neck surgery or plastic and reconstructive surgery. Because children may have craniofacial anomalies, including orofacial clefts, orthognathic problems, tumors, and blunt or penetrating trauma, such surgical management requires the ability to combine cosmesis, restoration of normal occlusion, and the promotion of normal growth and development of the entire facial skeleton (Kaban, 1993; Vig and Fields, 2000; Ord et al., 2002; Oza et al., 2002; Zeltser et al., 2003).
Clinical Settings for Pediatric Dentists
Most pediatric dental treatment occurs in the dental office without the need for psychological or pharmacologic intervention to address the child’s fear and anxiety. The hallmark of dental pain management is a kind practitioner and staff and the responsible use of adequate local or topical anesthesia, or both. For some patients, simple behavior modification techniques improve the level of cooperation in the dental chair. These techniques include the tell-show-do method and voice control for the fearful, hostile, or disruptive child. The tell-show-do technique involves explaining before the procedure, demonstrating the procedure outside of the child’s mouth, and then actually performing the procedure on the patient. This technique removes the fear of the unknown from the procedure (Lenchner and Wright, 1975). Voice control involves modulation of both the volume and tone of the dentist’s voice to achieve positive behavioral results (Wilson, 1994






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


