1. Capillary engorgement of the mucosa may occur throughout the respiratory tract, beginning early in the first trimester and increasing throughout pregnancy. Historically, a 6.0- to 6.5-mm (inner diameter) endotracheal tube has been recommended for intubation to decrease the possibility of airway trauma. However, the use of larger tubes may be possible in most patients should it be required. Fluid retention may lead to an enlarged tongue that may explain the increased prevalence of Mallampati class 3 and 4 airways in term parturients compared to the general population. Additionally, the airway exam may change during the course of labor resulting in a further increase in the airway class. Lastly, because of mucosal engorgement, nasotracheal intubation may cause epistaxis and is best avoided in pregnant women.
2. Minute ventilation increases by 45% to support the higher oxygen requirements of the mother and fetus and is driven by a proportional increase in tidal volume. As the pregnancy progresses, elevation of the diaphragm from the gravid uterus leads to 20% decrease in maternal functional residual capacity. The resultant decrease in oxygen reserve mandates adequate preoxygenation prior to induction of general anesthesia.
B. Cardiovascular System
1. Cardiac output increases progressively up to 50% from the end of the second trimester to term primarily due to increased stroke volume with a small contribution of increased heart rate. During labor, contractions of the engorged uterus provide a 300- to 500-mL autotransfusion into the maternal circulation, further increasing cardiac output. Cardiac output becomes highest immediately postpartum and may increase 80% to 100% above prelabor values due to further autotransfusion and loss of inferior vena cava (IVC) compression by the fetus. Despite the significant increase in cardiac output, blood pressure is not elevated at term from prepregnancy levels due to decreased peripheral vascular resistance.
2. Supine hypotension usually occurs after 20 weeks of gestation when the gravid uterus compresses the aorta and IVC of the patient in the supine position. Aortocaval compression decreases venous return and results in maternal hypotension and decreased uteroplacental blood flow. Providing left uterine displacement of 15 degrees when the patient is supine will mitigate this problem, with the potential for further increases in blood pressure and cardiac output at angles greater than 15 degrees.
C. Hematology
1. Blood volume increases markedly throughout the course of pregnancy. Because the plasma volume increases more than does red cell mass, a relative dilutional anemia occurs.
TABLE 32.1 Physiologic Changes Associated with Pregnancy
System
Parameters
Changes
Respiratory
Capacities/volume
Total lung capacity
-5%
Vital capacity
No change
Functional residual capacity
-20%
Inspiratory reserve volume
+5%
Expiratory reserve volume
-20%
Residual volume
-15
Closing capacity
No change
Tidal volume
+45%
Mechanics
FEV1
No change
FEV1/FVC
No change
Minute ventilation
+45%
Alveolar ventilation
+45%
Blood gases
PaCO2
-10%
PaO2
+5%-10%
pH
No change
HCO3
Decrease
Oxygen consumption
+20%
P50 at term
30 mm Hg
Cardiovascular
Cardiac output
+50%
Stroke volume
+25%
Heart rate
+20%-25%
Systematic vascular resistance
-20%
Hematology
Blood volume
+45%
Plasma volume
+55%
Red blood cell volume
+25%
Coagulation factors
Factors VII, VIII, IX, X, XII, fibrinogen
Increase
Prothrombin
No change
Factors XI, XIII
Decrease
Platelet count
No change or decrease
Total protein (albumin, globulin)
Decrease
Central nervous system
MAC
Decrease
Local anesthetic requirement
Decrease
Gastrointestinal
Gastric emptying
First trimester
No change
Second trimester
No change
Third trimester
No change
Labor
Decrease
Postpartum (18 h)
No change
Barrier pressure
First, second, third trimesters, labor
Decrease
Hepatic
AST, ALT, LDH, bilirubin
Increase
Alkaline phosphatase
Increase
Renal
Glomerular filtration rate
+50%
Renal plasma flow
+75%
2. The pregnant patient is hypercoagulable throughout gestation. The concentration of most coagulation factors increases in pregnancy as does platelet production, activation, and consumption. This hypercoagulable state helps to limit blood loss at delivery although it also increases the risk for thrombotic complications.
D. Nervous System
1. The minimum alveolar concentration (MAC) for inhalational anesthetics is decreased by 30% during pregnancy. The etiology is unclear but may be related to alterations of hormone and endorphin concentrations during pregnancy, which result in an increased pain threshold or pregnancy-induced analgesia. However, this increased sensitivity to volatiles may not translate to enhanced effect in the brain; therefore low MAC should be used with caution to avoid an increase in the incidence of awareness under anesthesia.
2. The local anesthetic dose required for regional anesthesia is reduced in the parturient compared to the patient who is not pregnant. Reasons for this include the following:
a. A decrease in cerebrospinal fluid (CSF) protein results in a greater proportion of free and active drug.
b. Elevated CSF pH increases the un-ionized fraction of the local anesthetic.
c. Distension of epidural veins during pregnancy results in a decrease in lumbar CSF volume with enhancement of local anesthetic spread and reduction of the segmental dose requirement for spinal anesthesia.
3. Sympathetic nervous system (SNS) activity increases from as early as 6 weeks of gestation despite decreases in diastolic pressure and total peripheral resistance. The parturient is highly dependent on the SNS for hemodynamic control, which is reflected by the significant decrease in blood pressure seen after regional anesthesia. SNS activity may return to normal by 36 to 48 hours postpartum.
4. The apex of lumbar lordosis is shifted cephalad with reduced thoracic kyphosis in the supine position. This may contribute to the increased cephalad spread of spinal anesthesia during pregnancy.
E. Gastrointestinal System. Because of the relaxation of the lower esophageal sphincter and mechanical displacement of the stomach by the gravid uterus, gastric reflux and heartburn are present in many pregnant patients. It is not clear when during the pregnancy the risk for aspiration increases, although the difference between intragastric pressure and lower esophageal sphincter tone is decreased as early as the first trimester. Gastric emptying is not delayed during pregnancy, but it is slowed during labor particularly following the administration of opioids. When a general anesthetic is planned, a nonparticulate antacid should be given routinely; a histamine (H2) blocker and metoclopramide should be considered. Patients in the second and third trimester should have a rapid sequence induction for general anesthesia.
F. Renal System. Renal plasma flow and glomerular filtration increases by up to 50%, leading to increased creatinine clearance and decreased blood urea nitrogen and serum creatinine levels.
G. Musculoskeletal. Increased lumbar lordosis and intra-abdominal pressure secondary to the enlarging uterus can stretch and compress the lateral femoral cutaneous nerve and produce a sensory loss over the anterolateral thigh (“meralgia paresthetica”). Carpal tunnel syndrome is common with a possible multifactorial etiology. Widening of the pubic symphysis is likely secondary to an increase in the hormone relaxin during pregnancy.
II. LABOR AND DELIVERY
A. Labor is defined as the onset of painful uterine contractions that lead to cervical change, and it may be divided into three stages.
1. The first stage begins with the onset of regular contractions and ends with full cervical dilation. It is divided into a slow latent phase and a rapidly progressive active phase characterized by accelerated cervical dilation. Patients with body mass index greater than 30 kg/m2 and male fetuses may experience prolonged first stage of labor. Such factors highlight the limitations of widespread use of a single labor curve for all patients.
2. The second stage extends from full cervical dilation until delivery of the infant.
3. The third stage begins after delivery of the infant, ending with delivery of the placenta.
B. Pain during the early first part of labor is primarily caused by uterine contractions and cervical dilation. Pain during the first portion of labor is mediated by the T10 to L1 segments of the spinal cord. In the active phase of the first stage of labor and in early second-stage labor, there is an additional component of pain due to perineal stretching that travels via the pudendal nerve to enter the spinal cord between the S2 and S4 segments.
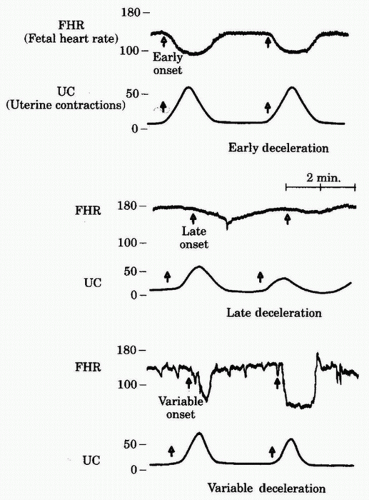
C. Intrapartum fetal evaluation is most commonly accomplished with fetal heart rate (FHR) monitoring—either continuous or intermittent. Continuous FHR monitoring is used in up to 85% of laboring patients in the United States. The normal FHR ranges from 110 to 160 beats per minute (bpm) over 10 minutes. Fetal tachycardia may signify fetal asphyxia, maternal fever, and/or chorioamnionitis or may be the result of maternally administered drugs. Persistent fetal bradycardia is most commonly due to hypoxia, but other etiologies include congenital heart block, maternally administered β-blockers, or hypothermia. FHR baseline variability is defined as the fluctuation in FHR of at least 2 bpm over an observed 10-minute period. Minimal variability refers to less than 5 bpm fluctuation, moderate ranges from 6 to 25 bpm, and marked greater than 25 bpm. It is modulated by fetal vagal tone and is a sign of underlying fetal health. Lack of variability must be interpreted in the context of FHR decelerations (decreases in FHR of 15 seconds or more from baseline to nadir). Recurrent concerning decelerations (late or deep variables), especially in the setting of minimal or absent variability, should prompt further evaluation to detect fetal compromise. Decelerations have been categorized (Fig. 32.1) as follows:
1. Early decelerations are gradual FHR decelerations that occur concomitantly with uterine contractions providing a mirror image of the uterine contraction, with the nadir of the deceleration occurring at the peak of the contraction. They are caused by an increase in fetal vagal tone, likely from mild hypoxia and compression of the fetal head, and do not require intervention.
2. By definition, variable decelerations are variable in both duration and appearance, and can occur spontaneously. Variable decelerations are associated with umbilical cord compression and decreased umbilical blood flow. They may indicate fetal compromise when severe and/or repetitive. Amnioinfusion (the instillation of amniotic fluid through a transcervical catheter after rupture of the fetal membranes) has been demonstrated to decrease the need for emergent cesarean delivery by improving or eliminating them.
3. Late decelerations are gradual decelerations that begin after the onset of a uterine contraction with a return of the FHR to the baseline only after the contraction has ended. Late decelerations suggest impaired maternal-fetal oxygen exchange and are triggered in susceptible fetuses by the decrease in fetal reserve with resulting intolerance of transient hypoxia. Medical interventions are tailored to improve placental oxygen delivery, among them left uterine displacement, correction of maternal hypotension, reconsideration of oxytocin dosing, and oxygen by face mask to the mother. A persistent late deceleration pattern might require delivery of the fetus.
FIGURE 32.1 Patterns of periodic FHR decelerations in relation to uterine contractions.
4. Electronic FHR monitoring has several significant limitations including a high rate of false positives and significant variability in its interpretation. Lastly, the use of electronic fetal monitoring has been associated with an increase in operative deliveries but has not resulted in a decrease in cerebral palsy rates. To minimize intervention based on false positives, additional ancillary tests may be considered:
a. Fetal scalp stimulation. A FHR acceleration in response to digital or instrumental stimulation of the fetal head is associated with a healthy nonacidotic fetus.
b. Fetal scalp blood pH determination is another method employed to evaluate the presence of fetal acidosis when abnormal FHR patterns cannot be corrected or their significance is unclear. In general, a pH above 7.25 is acceptable, and the labor may continue. A pH below 7.20 suggests that the fetus is acidotic and should be promptly delivered. If the pH is in the range of 7.20 to 7.25, close FHR monitoring and repeated scalp blood sampling are recommended.
c. Fetal pulse oximetry was designed to improve the assessment of the fetal status by continuously measuring fetal oxygen saturation in the setting of a nonreassuring FHR tracing. Unfortunately, studies have shown that the technology is not associated with a decrease in cesarean delivery rates or improvement in neonatal outcomes.
III. MEDICATIONS COMMONLY USED FOR LABOR AND DELIVERY
A. Vasopressors. Symptoms of maternal hypotension include light-headedness, nausea, difficulty breathing, and diaphoresis. Maternal hypotension may lead to decreased placental perfusion and fetal distress. Sympathetic blockade from regional anesthesia and decreased systemic vascular resistance may cause symptomatic maternal hypotension. An ideal vasopressor for obstetric anesthesia is one that increases both maternal blood pressure and placental blood flow.
1. Ephedrine is an indirect agonist of α– and β-adrenergic receptors. Its inotropic and chronotropic effects increase peripheral and uterine blood flow. Historically, ephedrine was the drug of choice for treatment of maternal hypotension.
2. Pure α1-adrenergic agents such as phenylephrine were previously believed to increase maternal blood pressure but decrease uteroplacental blood flow. Recent evidence indicates that judicious and precise dosing of phenylephrine is not associated with an increased incidence of fetal acidemia or decreased Apgar scores. Phenylephrine infusions have become increasingly common to prevent and treat maternal hypotension.
3. The more potent vasoconstrictors and inotropes such as norepinephrine and epinephrine are indicated for severe maternal hypotension resistant to volume resuscitation and traditional vasopressors.
B. Oxytocics or ecbolics are agents that stimulate uterine contractions.
1. Indications
a. To induce or augment labor
b. To control postpartum uterine atony and bleeding
c. To induce therapeutic abortion
2. The most frequently used drugs include the synthetic posterior pituitary hormone, oxytocin (Pitocin); the ergot alkaloids, ergonovine (Ergotrate) and methylergonovine (Methergine); and the prostaglandins, prostaglandin 15-methyl F2α (Hemabate) and prostaglandin E1 (misoprostol).
a. Oxytocin acts on the uterine smooth muscle to stimulate the frequency and force of contractions. Cardiovascular side effects of oxytocin include vasodilation, hypotension, tachycardia, and arrhythmias. In high doses, oxytocin may have an antidiuretic effect and produce hyponatremia, cerebral edema, and subsequent seizures. Recent evidence has suggested a possible association between oxytocin therapy and neurodevelopmental disorders. Oxytocin is routinely diluted and given by continuous intravenous (IV) infusion.
b. Ergot alkaloids control postpartum bleeding following the third stage of labor. Side effects include systemic vasoconstriction and hypertension, which may be amplified in the presence of vasopressors. IV injection has been associated with severe hypertension, seizures, stroke, myocardial infarction, and pulmonary edema. Intramuscular (IM) administration is therefore highly recommended. Ergot alkaloids should be used with caution or avoided in patients with peripheral vascular disease, preeclampsia, hypertension, or coronary artery disease.
c. Prostaglandin 15-methyl F2αis a treatment for uterine atony. The usual dose is 250µg IM or intramyometrially, not more frequently than every 15 minutes, with a total maximum dose of 2 mg. Transient hypertension, severe bronchoconstriction, and increased pulmonary vascular resistance have been reported, contraindicating its use in patients with a history of asthma. Fever, nausea, vomiting, and diarrhea are additional side effects.
Only gold members can continue reading. Log In or Register to continue