2.3 Anatomy of the pelvic floor
There is increasing evidence that the pelvic floor muscles (PFM) perform multiple functions such as: continence and pelvic organ support (DeLancey 1990, Howard et al. 2000); sexual function (Baytur et al. 2005); respiration (Hodges et al. 2007); spinal stability; and containment of intra-abdominal pressure (IAP) (Hemborg et al. 1985, Pool-Goudzwaard et al. 2004, Smith et al. 2008). The physiological mechanisms by which they perform these roles are not clearly understood, predominately due to a lack of suitable instrumentation. The pelvic floor (PF) remains, particularly from a biomechanical perspective, an understudied region of the body (Ashton-Miller & DeLancey 2007). PF dysfunction for certain encompasses both urinary and faecal incontinence, pelvic organ prolapse (POP) and pelvic pain (Martins et al. 2007). It is a significant problem for both women and men and has been termed the hidden epidemic (DeLancey 2005), with estimates in the USA indicating that between 21% and 26% of American women have at least one PF disorder, with the greatest percentage experiencing urinary incontinence (Nygaard et al. 2008). PF dysfunction affects between 300 000 and 400 000 American women so severely that they require surgery, and 30% of those will require re-operations (Olsen et al. 1997, Boyles et al. 2003). Similar prevalence data of PF dysfunction are currently unavailable in the UK.
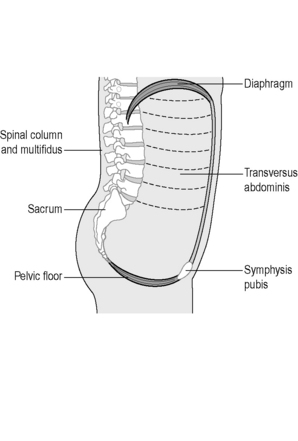
A combination of neuropathic changes, muscle, fascial or connective tissue damage is most likely responsible for the development of PF disorders yet the precise mechanisms remain controversial (Shafik et al. 2005, Ashton-Miller & DeLancey 2007, Petros 2007, Smith et al. 2007). The PF is an intricate, complicated structure, and by virtue of its anatomical position makes it a challenging area to study. The support mechanisms of the PF are responsible for the maintenance of continence and prevention of POP during rises of IAP (Ashton-Miller & DeLancey 2007), so functionally it not only has to allow the passage of urine and faeces at the appropriate time, it must also prevent incontinence. The PF is essential for sexual activity, conception, fertility and vaginal delivery (Herschorn 2004, Delancey 2005). More recently the PF has been implicated in contributing to spinal stability and respiration (Hodges et al. 2007). The lumbopelvic cylinder is closed inferiorly by the PF, the respiratory diaphragm forms the top, the transversus abdominis the sides and the spinal column runs through the middle, supported posteriorly by segmental attachments of lumbar multifidus, anteriorly by segmental attachments of psoas and the abdominal muscles (Figure 2.3.1).
The following sections describe the gross anatomy of the PF and organs. Further details and a practical PF anatomy guide for the palpating physician can be found in Chapter 13.
Pelvic floor muscles
The PFM is the collective name for the muscles of the PF; unfortunately throughout the literature, there still remains lack of consensus regarding their description and terminology. A recent review of the literature revealed over 16 different overlapping terms for different parts of the muscle, yet the anatomy was found to be very consistent amongst different studies (Kearney et al. 2004). Kearney et al. concluded that confusion could be limited by standardizing terminology based upon origin and insertion points of the muscle. Therefore, for the purposes of this book, wherever possible, nomenclature is based upon origin-insertion (attachment) points.
The deep PFM: Levator ani muscle
The pubovisceral muscle is a thick U-shaped muscle which arises from the pubic bones on either side of the midline, and a band of fascia, the arcus tendineus levator ani (ATLA), laterally (Figure 2.3.2).
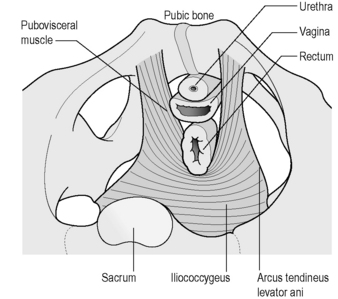
Figure 2.3.2 Levator ani muscle seen from above.
Adapted, with permission from Elsevier North-Holland, from Kearney et al. (2004). © DeLancey 2003).
It passes behind the rectum forming a sling-like arrangement, attaching to the walls of the vagina, or fascial sheath of the prostate and urethra in the male, the perineal body and anal sphincter. The pubovisceral muscle can then be divided into three main components based upon the anatomical attachments: puborectalis, pubovaginalis or levator prostate in the male and pubococcygeus (Figure 2.3.3). In the female, the puborectalis portion passes beside the vagina with some attachment to the lateral vaginal walls. Some other fibres insert into the rectum, and others pass behind the anorectal junction. The fibres of the pubovaginalis pass between the vagina and pubis, connecting to the fascia that supports the urethra. Pubococcygeus only comprises a small proportion of the levator complex, although clinicians have often referred to the entire pubovisceral muscle as pubococcygeus. Its fibres pass from the pubic bones to the coccyx, with some extending behind the rectum and to the anal canal.
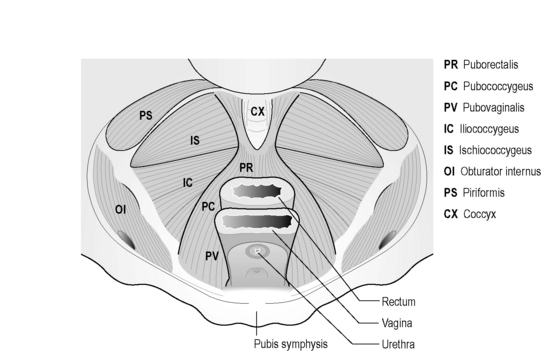
The ischiococcygeus is not technically part of the PFM, but forms the remainder of the pelvic diaphragm posteriorly, attaching to the ischial spine, the coccyx and lower part of the sacrum (Figure 2.3.3).
The superficial PFM and perineal body
Along with the connective tissue membrane surrounding them, the superficial PFM is often called the perineal membrane or urogenital diaphragm (Figures 2.3.4, 2.3.5). In the female, the perineal membrane lies level with the hymenal ring and attaches the urethra, vagina and perineal body to the ischiopubic rami.
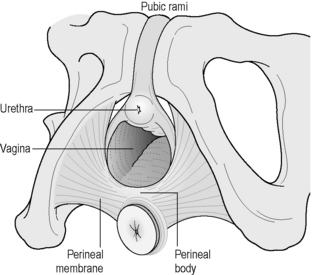
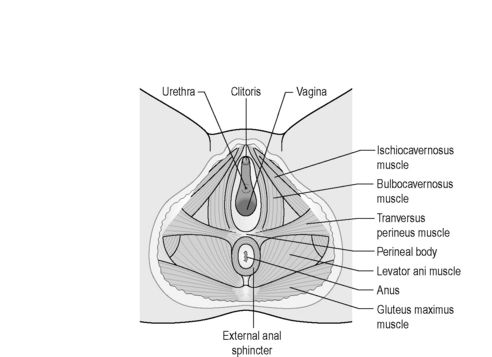
Figure 2.3.5 Superficial muscles of the pelvic floor.
Reproduced from Drake (2009) Gray’s Anatomy Student Edition, Churchill Livingston.
The perineal body is a fibromuscular structure containing smooth muscle, elastic fibres and nerve endings in the middle of the perineum, between the urogenital and anal hiatuses (Figures 2.3.4, 2.3.5). Fibres of the rectum and anal sphincter, superficial PFM and levator ani also extend into the perineal body (Herschorn 2004). There is no consensus over the anatomical configuration of these muscles and fascia (Oelrich 1983, DeLancey 1999) yet the striated muscle fibres are generally thought of as the transverse perinei superficialis, urogenital sphincters (compressor urethrae, urethrovaginal) and external anal sphincters (Figures 2.3.4, 2.3.5, 2.3.6). The bulbocavernous and ischiocavernosus are the most superficial layer of the PF and have a mainly sexual function (Peschers & DeLancey 2008).
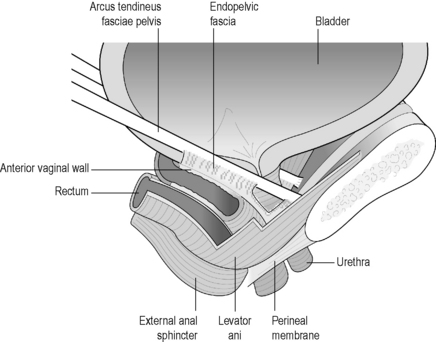
Endopelvic fascia
Related posts:
 Psychophysiology and pelvic pain
Psychophysiology and pelvic pain
 8.2: Interdisciplinary management of chronic pelvic pain: A US physical medicine perspective
8.2: Interdisciplinary management of chronic pelvic pain: A US physical medicine perspective
 Electrotherapy and hydrotherapy in chronic pelvic pain
Electrotherapy and hydrotherapy in chronic pelvic pain
 Intramuscular manual therapy: Dry needling
Intramuscular manual therapy: Dry needling
 Patients with pelvic girdle pain: An osteopathic perspective
Patients with pelvic girdle pain: An osteopathic perspective
 Practical anatomy, examination, palpation and manual therapy release techniques for the pelvic floor
Practical anatomy, examination, palpation and manual therapy release techniques for the pelvic floor
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


