Anatomy of Muscles, Tendons, Joints, Blood Vessels, and Meninges
Lars Edvinsson
Marc Abel
Vital organs of the body are encased by the skeletal system, either completely or in association with elements of connective tissue and the muscular system. The brain is completely surrounded by the bones of the skull. The spinal cord is almost completely protected by bony parts of the vertebrae, although some apertures are filled by strong connective membranes or ligaments. The contraction of a muscle would be ineffectual if one end were not firmly attached to the fixed portion of the skeletal system and the other end equally firmly attached to the skeletal member of the body part to be moved.
THE SKULL
The skull bones may be divided into two groups: those forming the cranium (the “brain box”) and those forming the face. The cranial bones enclose the cranial cavity, which is divided into anterior, middle, and posterior portions. The bones of the face form mainly the anterior part of the skull. The primary function of the skull is to protect the brain and the associated organs for vision, hearing, taste, and smell. It also provides attachment for many of the muscles of the head and neck.
Although it is thought of as a single bone, the skull is composed of 28 separate bones. Many of these bones are considered to be flat, consisting of two thin plates of compact bones enclosing a narrow layer of cancellous bone. In terms of shape, however, the bones are far from flat and can show pronounced curvatures. Diploe is used to describe the cancellous bone within the flat bones of the skull.
One may also subdivide the skull into neurocranium and viscerocranium. In humans, the neurocranium is extraordinarily large. The very size and dominance of the human brain emphasizes the skull’s cerebral function, overshadowing others. Even in this limited role, the cranium cannot be considered merely protective. Sporadic protection of the brain from external impacts is of undoubted value; the need for a barrier against stresses from the play of powerful masticatory and axial musculature is less obvious, but continual. In addition to these extraneous forces, the rigid cranial walls provide continuous isolation for the cerebral circulation. Moreover, the reputed buffering by meninges, subarachnoid space, and contained fluid could be effective only within a rigid container.
The brain’s dependence on uninterrupted blood flow is well known; independence of cerebral arterial pressure from extracranial variations, caused by some form of autoregulation, the basic nature of which is still unidentified, is also well established (5). It appears likely that localization of a brain in a rigidly maintained space is a factor in such mechanisms, despite lack of precise evidence. However, the cranial cavity is not closed. Cerebrospinal fluid passes freely through the foramen magnum, displaceable in either direction. Variability in volume of fluid in the cerebral ventricular system and numerous connections between intra-and extracerebral veins add to the complexity of the fluid circulation. Nevertheless, it appears undeniable that enclosure of the brain in an otherwise invariable space must be a crucial factor in the control of the cerebral circulation.
THE CERVICAL VERTEBRAE
This part of the vertebral column is extremely flexible, permitting a wide range of movements of the head and neck. The seven cervical vertebrae are smaller than those lower
in the column; however, the main distinguishing characteristic is the presence of three foramina instead of one. In addition to the usual vertebral foramen, there is an opening in each transverse process called the transverse foramen (Fig. 9-1), through which pass the vertebral arteries on their way to the brain.
in the column; however, the main distinguishing characteristic is the presence of three foramina instead of one. In addition to the usual vertebral foramen, there is an opening in each transverse process called the transverse foramen (Fig. 9-1), through which pass the vertebral arteries on their way to the brain.
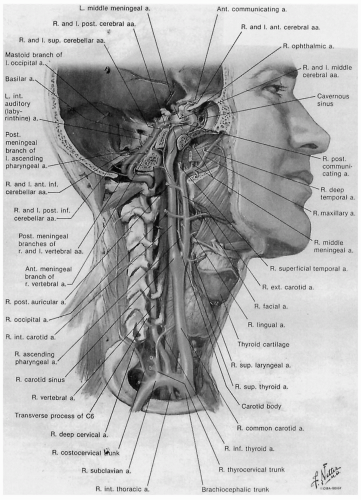 FIGURE 9-1. Arteries to the brain and meninges. |
The first two cervical vertebrae have additional distinctive features and have been given specific names. The atlas, or the first cervical vertebra, supports the head. Having no body or spinous process, it is little more than a bony ring, which receives, on its superior articular surface, the condyles of the occipital bone. By means of this joint, one is able to rock the skull back and forth, as in nodding agreement. The second cervical vertebra is called the axis, and is easily identified by the presence of the odontoid process, which arises from the body. This process fits up into the anterior part of the atlas and forms the axis of rotation. The seventh cervical vertebra has a very prominent spinous process, which can be felt at the nape of the neck.
THE JOINTS OF THE CERVICAL VERTEBRAE
The joints of the cervical vertebra, with the exception of the specialized joints between atlas and axis, are arranged on a common plane (Fig. 9-2). The vertebral bodies, united by intervertebral fibrocartilaginous discs, form a series of nonsynovial, cartilaginous joints. The intervertebral discs, because of their pliability, provide flexibility to the vertebral column and function as shock absorbers. The disc consists of a tough outer fibrocartilaginous ring, the annulus fibrosus, and inside a gelatinous mass, the nucleus pulposus. The amount of movement at a single joint is not great, but the range of movement in the entire series is considerable. Gliding movement also occurs at each of the synovial joints between articular processes of adjacent vertebrae.
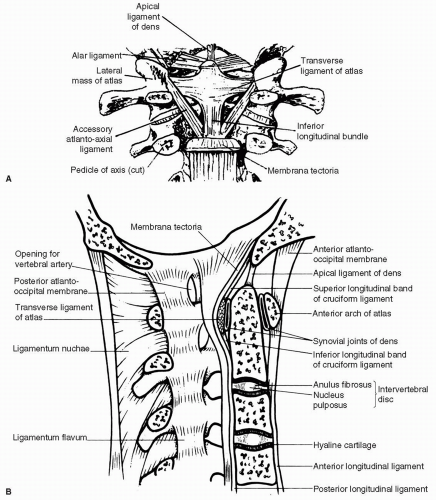 FIGURE 9-2. A: Dissection from behind to show the main ligaments that connect the occipital bone, atlas, and axis. B: Median sagittal section through the base of the skull and the upper cervical vertebrae to illustrate some of the vertebral joints and ligaments. |
The joints are strengthened by anterior and posterior ligaments (see Fig. 9-2). These run in the midline along the anterior and posterior surfaces of the bodies of the vertebrae. They are attached to the intervertebral discs. The anterior longitudinal ligament is stronger and is attached
above to the anterior tubercle of the atlas and to the basilar part of the occipital bone. The posterior longitudinal ligament runs inside the vertebral canal and is attached above to the body of the axis.
above to the anterior tubercle of the atlas and to the basilar part of the occipital bone. The posterior longitudinal ligament runs inside the vertebral canal and is attached above to the body of the axis.
THE JOINTS BETWEEN THE VERTEBRAE
The articular facets of adjacent vertebrae are united by synovial joints (see Fig. 9-2). Concerning the ligaments associated with the vertebral arches passing between adjacent laminae is the ligamentum flavum. This is composed primarily of elastic fibers. Whereas the tips of the spinous processes in other parts of the vertebral column are joined by interspinous and supraspinous ligaments, these are poorly developed in the cervical region, and the ligamentum nuchae is present. This is a triangular, fibroelastic septum lying between the postvertebral muscles in the midline. Its posterior border extends from the external occipital protuberance to the spinal aspect of the seventh cervical vertebra. Its anterior border is attached to the spines of the cervical vertebrae and to the posterior tubercle of the atlas. Its superior border is attached to the external occipital crest. The movements of the vertebral column are described as flexion, extension, lateral flexion, and rotation.
ATLANTOOCCIPITAL JOINTS
The two atlantooccipital joints between the occipital condyles and the superior articular facets of the atlas are uniaxial synovial joints placed on either side of the foramen magnum (see Fig. 9-2). The anterior and posterior atlantooccipital membranes, attached to the edge of the foramen magnum superiorly and to the arch of the atlas inferiorly, strengthen the joints. Movement, occurring around a transverse axis, results in nodding or flexion and extension of the head.
ATLANTOAXIAL JOINTS
The atlantoaxial joints are a pair of synovial joints between the articular processes of the first and second cervical vertebrae (atlas and axis, respectively) and two median synovial joints formed by the articulation of the dens of the axis anteriorly with the anterior arch of the atlas and posteriorly with the transverse ligament. The transverse ligament of the atlas is a stout band of connective tissue that passes posterior to the dens and attaches to the medial aspect of the lateral masses of the atlas. From the middle of the transverse ligament, longitudinal fibers pass superiorly to insert into the anterior edge of the foramen magnum and inferiorly to attach to the posterior surface of the body of the axis. These longitudinal bands, together with the transverse ligament, form the cruciate ligament of the atlas. The axis is directly attached to the occipital bone by the apical and alar ligaments, which arise from the tip and either side of the dens, respectively.
Rotary movements of the head occur between the atlas and axis. Movement is free. However, the alar ligaments limit rotation of the skull and atlas on the axis, and the apical ligament tightens during extension.
MUSCLES OF THE HEAD AND NECK
The head is balanced atop the axial skeleton in the erect anatomic position. It is held in this balanced position partly by its own weight pressing down on the atlantooccipital joint and partly by the coordinated action of the muscles that approach the base of the skull from all directions. The action of antagonists is important in movements of the head and neck because frequently a movement, once started, is largely completed by gravity. The antagonists then have the role of regulating the gravity movement and checking it at the appropriate point. For example, when the head and the neck are bent forward in flexion, the muscles extend to allow the forward fall of the head produced by gravity. If the body is in the supine position, however, gravity tends to resist flexion of the head, which then can be performed only by active concentration of muscles that can produce flexion.
The mobility of the cervical part of the vertebral column greatly extends the range of motion of the head. It will be found that many of the muscles that produce movements of the neck also move the head either by direct attachments to the skull or because the head is carried along as the neck is moved in various directions.
Muscles Moving the Head Alone
The head alone can be moved without accompanying movements of the neck. Several small short muscles under the base of the skull are grouped together as the suboccipital muscles. There are also several other muscles that run longer, independent courses to move the head.
Suboccipital Muscles
Suboccipital muscles are clustered together in a ring formation immediately below the base of the skull (Fig. 9-3). They run a short course from attachments on the atlas or axis to the occipital bone of the skull or, in one case, from the axis to the atlas. These muscles usually work together
to extend or flex the skull by a rocking motion of the occipital condyles on the atlas or to rotate the skull and atlas together around the pivot joint with the axis. The short, quick, almost automatic movements of the head in following movements of the eyes are largely the function of these muscles.
to extend or flex the skull by a rocking motion of the occipital condyles on the atlas or to rotate the skull and atlas together around the pivot joint with the axis. The short, quick, almost automatic movements of the head in following movements of the eyes are largely the function of these muscles.
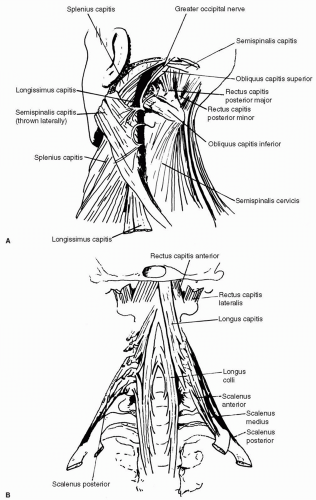 FIGURE 9-3. A: Suboccipital triangle of the left side. B: Prevertebral and scalene muscles. |
Sternocleidomastoid Muscle
A long, straplike muscle crosses the neck obliquely from origins on both the anterior surface of the manubrium and the medial one third of the clavicle as it ascends to insert upon the mastoid process of the skull. The action of the
sternocleidomastoid muscle is to pull the skull downward on the same side and to draw it forward. The result is that the head is tilted to the same side and, at the same time, the face is rotated toward the opposite side. The tendinous origin of the two muscles can be felt diverging at the base of the neck above the sternum where they outline the suprasternal fossa. When one’s head is turned to the right, the taut borders of the muscle on the left can be followed obliquely upward to its insertion. If both muscles act at the same time, there can be no turning of the head because the muscles oppose each other. Flexion of the head will result instead, particularly when the body is supine and it is necessary to raise the head, as from a pillow, against the resistance of gravity.
sternocleidomastoid muscle is to pull the skull downward on the same side and to draw it forward. The result is that the head is tilted to the same side and, at the same time, the face is rotated toward the opposite side. The tendinous origin of the two muscles can be felt diverging at the base of the neck above the sternum where they outline the suprasternal fossa. When one’s head is turned to the right, the taut borders of the muscle on the left can be followed obliquely upward to its insertion. If both muscles act at the same time, there can be no turning of the head because the muscles oppose each other. Flexion of the head will result instead, particularly when the body is supine and it is necessary to raise the head, as from a pillow, against the resistance of gravity.
Associated Muscles
A long series of deep muscles, closely related to the vertebral column, exists to produce movement of the axial skeleton. The most superior of these deep muscles extend between the cervical vertebrae and the skull. Although their parent muscle masses are concerned with movements of the vertebral column, the following compartments move the head in company with those movements. It should be remembered that, when they act, other muscles are producing movements of the neck or the entire back.
Anterior Muscles
The longus capitis is a thin muscle that arises from the transverse process of the third to the sixth cervical vertebrae. It runs upward along the front and sides of the upper cervical vertebrae to insert on the base of the skull in front of the rectus capitis anterior. Its action, similar to that of its suboccipital companion, is that of flexion of the head.
Posterior Muscles
Posteriorly located along the vertebral column are the superior portions of the deep back muscles. The longissimus capitis and the semispinalis capitis continue the long column of muscles upward to the skull, where they attach to the posterior aspect of the base of the skull, overlapping the posterior suboccipital muscle (see Fig. 9-3A). The splenius muscle, which runs from the thoracic spinous processes to the cervical transverse processes, has a part, the splenius capitis, that extends from the ligamentum nuchae of the cervical vertebrae upward and laterally to attach behind the sternocleidomastoid muscle on the mastoid process. All these muscles control the forward fall of the head with gravity in flexion and, as the head extends, bring it back from the flexed position to its normal attitude.
Muscles That Move the Neck
The neck is moved by muscles located anterior or posterior to the bodies of the cervical vertebrae. These muscles have their lower attachments to the axial skeleton below the neck.
Scalene Muscles
Three slender fusiform muscles descend obliquely laterally from attachments to the anterior surface of the transverse processes of the cervical vertebrae to the first or second rib (see Fig. 9-3B). These muscles add a minor contribution to the stability and elevation of ribs during respiration. The scalenus muscles have an anteroposterior relationship to each other and thus are named the scalenus anterior, medius, and posterior. They are active in lateral flexion of the neck but, combining forward in their descent, can also contribute to forward bending. It should be noted, however, that the sternocleidomastoid muscle, while pulling on the head, is powerful in lateral flexion of the neck. The two sternocleidomastoid muscles acting together are stronger in flexion of the head and neck than the scalenes.
The longissimus cervicis is primarily a flexor muscle of the neck. It is a flat muscle, running along the sides and the front of the cervical vertebrae.
Associated Muscles
The long posterior muscle masses of the deep back muscles have attachments to the back of the neck. Cervical portions of the longissimus, semispinalis, and splenius muscles described with the head muscles form a group of posterior cervical muscles. These act with the muscles of the back to control flexion of the neck and to return the flexed neck and the head to the upright position.
Two sets of muscles are related to the hyoid bone, which is unarticulated to the rest of the skeleton and is located in the neck between the mandible and the larynx. The muscles that attach to the hyoid bone are called the suprahyoid and the infrahyoid muscle because of their positional relationship to the bone (see below). The infrahyoid muscles anchor the hyoid bone against the pull of the suprahyoid muscles, which use the bone for their lower attachment. The suprahyoid muscles form or shape the floor of the mouth. All use the hyoid bone for their lower attachment and, therefore, depend on the contraction of the infrahyoid muscles to provide a fixator action on the hyoid bone.
Muscles Associated With the Hyoid Bone
These muscles are grouped according to their position relative to the hyoid bone. Most are named by their origin and insertion and contribute to the movements that
occur when we swallow. The suprahyoid muscles (above the hyoid bone) include:
occur when we swallow. The suprahyoid muscles (above the hyoid bone) include:
The digasticus, consisting of two portions or bellies. The posterior belly draws the hyoid backward; the anterior belly draws it forward,
The stylohyoid draws the hyoid bone up and back.
The mylohyoid forms the floor of the mouth. It lies between the limbs of the mandibular body and raises the hyoid bone and tongue.
The geniohyoid, located superior to the mylohyoid, reinforces the floor of the mouth.
The infrahyoid muscles (below the hyoid bone) include:
Sternohyoid draws the hyoid downward.
Sternothyroid draws the larynx downward.
Thyreohyoid draws the larynx upward if the hyoid is fixed.
Omohyoid draws the hyoid downward.
Facial Muscles
Facial muscles are the muscles of facial expression. Their contractions move the fleshy parts of the face for speech and cause the various expressions associated with emotions and feelings. Some of the facial muscles are as follows:
Orbicularis oculi encircles the eye and closes or winks the eye.
Orbicularis oris encircles the mouth and closes and protrudes the lips.
Levator labii superioris elevates the upper lip to give an expression of contempt.
Zygomaticus draws the corners of the mouth up and back, as in smiling.
Risorius draws the corners of the mouth directly sideways, as in a grimace.
Triangularis draws the corners of the mouth down and back to create an expression of sadness.
Depressor labii inferioris depresses the lower lip.
Mentalis elevates the lower lip and protrudes it, as in pouting.
Buccinator lies beneath the muscles listed above and compresses the cheek. It is sometimes called the trumpeter’s muscle because it is used intensively in playing a brass musical instrument like a trumpet.
Corrugator produces frown lines in the central forehead.
Cranial Muscles
The cranial muscles lie on the forehead, on the back of the head, and around the ears. The epicranius covers the sides and top of the skull. It is divided into an occipitofrontal group consisting of an anterior frontalis and posterior occipitalis and a temporoparietal group consisting of the auricular muscles. The occipitalis and frontalis attach to a broad, flat tendon (galea aponeurotica) over the top of the skull. The frontalis pulls the scalp forward, and the occipitalis draws the scalp backward.
MUSCLES OF MASTICATION
The muscles of mastication are the muscles acting on the temporomandibular joint to close the jaws. The masticatory muscles are intensely strong. They produce the major power to forcibly close the jaws, to clench the teeth, and to grind food. These muscles protrude and retract the mandible and move it from side to side. In contrast to the action of the masticatory muscles, opening of the jaws is largely the result of gravity during inhibition of masticatory muscle action, assisted by the contraction of the suprahyoid and platysma muscles.
Four muscles are most important in mastication. The temporalis fills a depression on the side of the skull and elevates the mandible, closing the mouth. The masseter covering the ramus of the mandible is the most powerful jaw-closing muscle. Both temporalis and masseter can be felt contracting with clenching of the jaws and feeling the skull in the appropriate area. The medial pterygoid is internal to the mandibular ramus and elevates the jaw; the lateral pterygoid lies between the medial pterygoid and the ramus and depresses the mandible, opening the jaw (mouth). The pterygoids also move the mandible laterally.
Muscles Associated With the Hyoid Bone
These muscles may be grouped according to their position relative to the hyoid bone. Most are named by their origin and insertion, and contribute to the movements that occur during swallowing. The suprahyoid muscles (above the hyoid bone) include the digasticus, consisting of two portions or bellies. The posterior belly draws the hyoid backward; the anterior belly draws it forward. The stylohyoid draws the hyoid bone up and back. The myelohyoid forms the floor of the mouth. It lies between the limbs of the mandibular body and raises the hyoid bone and tongue. The infrahyoid muscles (below the hyoid bone) are as follows:
Sternohyoid draws the hyoid downward.
Sternothyroid draws the larynx downward.
Thyreohyoid draws the larynx upward if the hyoid is fixed.
Omohyoid draws the hyoid downward.
Neck Muscles
The muscles of the neck consist of two superficial muscles on the anterior neck and a number of deep muscles that attach to the vertebrae and the skull.
Superficial Muscles
The platysma is a broad sheet covering the inner side of the shoulder and lateral neck and mandible. It draws the corners of the mouth down and sideways as in screaming or in an expression of horror. The sternocleidomastoid was discussed previously.
Deep Muscles
These are divided into anterior, lateral, and posterior groups. The anterior group includes the longus colli, longus capitis, and rectus capitis, all of which flex the neck on the chest. The lateral group includes the three scalenes, which bend the neck to the side and help to elevate the ribs if the neck is fixed. The posterior group includes the semispinalis, longissimus, and splenius, which extend the neck and raise the chin.
Possible Movements
The column may be flexed or bent forward, extended or bent backward, abducted or bent to the side, adducted or returned to the midline, and rotated or twisted. Some of the muscles responsible for these actions also have other functions in the overall movement of the spinal column, but they are not described in detail in this chapter.
MUSCLES PROVIDING FACIAL EXPRESSION
A group of thin muscles that are closely applied to the scalp and to the face have developed primarily to move the scalp or to guard the opening of the skull. The contraction of these muscles also produces characteristic movements of the face in the display of emotion. The many small muscles beneath the skin of the scalp and face, particularly around the eyes and mouth, alter facial expression, a very important means of communication.
The epicranius (occipitofrontalis) is a broad musculofibrous sheet that covers the top and the sides of the skull (see above). It is composed of two muscular portions, the frontalis and the occipitalis, connected by a fibrous sheet called the epicranial aponeurosis or galea aponeurotica. The frontal fibers of the muscle extend over the forehead to insert by blending of these fibers with facial muscles that encircle the orbits or cover the root of the nose. The occipital fibers draw the scalp backward; the frontal fibers draw it forward. The frontal portion also wrinkles the forehead and raises the eyebrows.
Facial movements and the variety of facial expressions are largely the byproducts of the action of muscles that exist primarily to guard the orifices of the orbits, nose, and mouth. The muscles responsible for the protection of these openings act as sphincters or dilators to control the degree of opening or closing of the eyelids, nostrils, or lips.
The orbicularis oculi keeps the lid closely applied to the eyeball, closes the eyes, and draws down the eyebrow. The orbicularis oris lies within the lips and is the sphincter of the mouth. The other muscles associated with the lips have been variously named and subdivided but are not described in this chapter.
The buccinator muscle arises from the side of the maxilla superiorly, from the inner surface of the mandible inferiorly, and from the pterygomandibular raphe, which is a dense band of the deep fascia of the pharynx. The buccinator thus constitutes the essential muscular coat of the cheek and is inserted into the corner of the mouth. The buccinator aids in chewing movements by keeping the cheek more firmly in contact with the teeth, preventing food from being pocketed between teeth and cheek.
All the muscles of the scalp and of facial expression are innervated by the seventh cranial nerve, the facial nerve, except for the levator palpebrae superior. Because the facial nerve is the sole nerve supply of many facial muscles, disease or injury affecting it has widespread cosmetic and functional effects.
NERVE SUPPLY TO THE HEAD AND NECK
Nerves of the Face
Both motor and sensory nerves are found on the face. The motor nerves are derived from the facial nerve (cranial nerve VII). Although the facial nerve contributes somewhat, the sensory innervation is primarily from the three divisions of the trigeminal nerve, with a small contribution from the cervical plexus via the great auricular nerve. The brain gives rise to 12 pairs of cranial nerves, which supply motor and sensory fibers to structures in the head, neck, and shoulder regions. Each cranial nerve varies in the components it carries, depending on the structures innervated.
Several of the cranial nerves, specifically IV, VI, XI, and XII, although supplying striated muscles, do not contain any demonstrable sensory fibers. It is generally accepted that sensory fibers from these muscles are conveyed to the central nervous system by branches of the trigeminal nerve (cranial nerve V). Because of its widespread sensory distribution, both superficial and deep, the trigeminal nerve is often described as the great sensory nerve of the head. The trigeminal nerve is the largest cranial nerve. It supplies sensory fibers to the anterior cranium and face and motor fibers to the chewing muscles. Ophthalmic, maxillary, and mandibular branches form the nerve and supply sensory fibers to all structures within their distribution (Fig. 9-4).
Related posts:
 Principles of Clinical Pharmacology, Randomized Controlled Clinical Trials, and Evidence-Based Medicine in Headache
Principles of Clinical Pharmacology, Randomized Controlled Clinical Trials, and Evidence-Based Medicine in Headache
 Calcitonin Gene-Related Peptide and Other Peptides
Calcitonin Gene-Related Peptide and Other Peptides
 The Migraines: Introduction
The Migraines: Introduction
 Channelopathies and Their Possible Relation to Migraines
Channelopathies and Their Possible Relation to Migraines
 Autonomic Dysfunction in Migraines
Autonomic Dysfunction in Migraines
 Psychological and Behavioral Treatments of Migraines
Psychological and Behavioral Treatments of Migraines
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


