CHAPTER 1 Local anaesthesia
Pharmacology

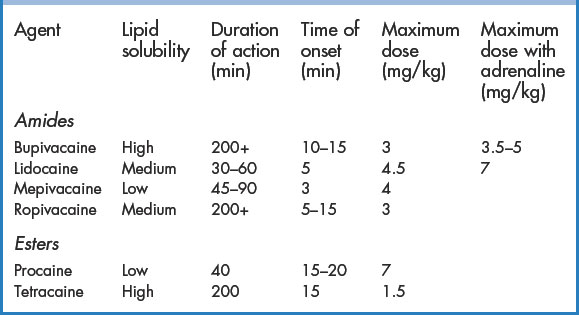
There are many local anaesthetics readily available in clinical practice (Table 1.1). The most widely used agents include lidocaine and bupivacaine. Local anaesthetics are most commonly used during wound repair and for minor procedures (drainage of abscesses etc.). Techniques for their administration in the ED include topical application, local infiltration, field block, and peripheral nerve block. Lidocaine, the most commonly used local anaesthetic, is inexpensive and is available in a variety of concentrations (1% and 2%) and volumes (20-mL vials, 5-mL ampoules, and 1.8-mL dental cartridges). Some formulations are appropriate for subcutaneous administration only. Only the IV preparation should be used for intravenous regional anaesthesia and haematoma blocks. The combination of 1% or 2% lidocaine with adrenaline in a ratio of 1:80 000 (found in dental cartridges or premixed vials) produces optimal skin vasoconstriction and adequate duration of effect for most procedures. If premixed solutions are not available, the addition of 0.1 mL of adrenaline 1:1000 to 10 mL of lidocaine will create a 1:100 000 solution. Bupivacaine has a much longer duration of action than lidocaine and therefore may be more appropriate for very complex wounds requiring long repair times or when prolonged post-procedure analgesia is required. In settings where wound care may be interrupted (in a busy ED), the use of bupivacaine may avoid the need for further administration of local anaesthesia to complete a wound repair. For these reasons, many ED physicians choose bupivacaine or ropivacaine over lidocaine. A mixture of the two agents is often used because of the rapid onset of lidocaine and the longer duration of bupivacaine and to increase the volume of injected agent for regional anaesthesia. Studies have suggested that bupivacaine is underused in the ED, mostly because it is unfamiliar or because doctors have misconceptions about its onset of action or safety. It is an excellent local anaesthetic for the ED!
Adverse events
Toxic adverse events are dose related; therefore, the maximum dose for any agent should not be exceeded (Table 1.1). Adverse reactions involve the central nervous system (CNS) and, to a lesser degree, the cardiovascular system (CVS).
Decreasing the pain of local anaesthesia
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


