12
Aggression
Introduction
Violence and aggression is recognized as a major hazard for staff within the healthcare sector (Chuo et al. 2012a). The fields of mental health, learning disability and emergency care, unsurprisingly, report the highest incidence of verbal and physical threats to staff (Health & Safety Commission Advisory 1997). The regular occurrence of violence within the NHS has been frequently documented (Crilly et al. 2004, Whittington & Winstanley 2008). A review of the management of work-related violence by the Royal College of Nursing (2008) suggested that the impact of work-related violence and aggression is not only physical in terms of injuries sustained by an individual, but can also result in psychological harm that may lead to stress, burn-out, anxiety and depression. These effects can, in turn, lead to a diminished job satisfaction, lower commitment to work and increasing levels of absence for the individual, which clearly impacts on the NHS as an organization.
While far from being the only area within the general hospital setting to see a rise in aggression and violence, the growing level of aggression witnessed within the emergency care setting is also well documented (Atawnehet et al. 2003, Crilly et al. 2004). Standing & Nicolini (1997) argued that the highest risks of violence at work are associated with:
• working with confused older people
• working with those who have mental health problems
• handling valuables or medication
In a study of the psychological impact of violence on staff, Hislop & Melby (2003) found that emergency nurses who had experienced violence in their departments expressed feelings of frustration, anger and fear as a result of this. The Scottish Government recognized the growing number of aggressive and violent incidents being perpetrated against emergency care staff, introducing new legislation, the Emergency Workers (Scotland) Act (2005) aimed at offering some protection for staff in this area. Although prevention of aggression and violence in the Emergency Department (ED) is the aim, it may not always be possible to stop this occurring. Aggression and violence in the ED develops as a result of a wide variety of factors, some of which can be identified and managed within the clinical setting. Others are unfortunately beyond the control of the emergency care staff; however, their awareness of these factors and the appropriate strategies to manage these issues is vital to maintain a safe environment for both staff and patients. This chapter will discuss the problem from these perspectives and offer some suggestions to assist the emergency nurse to resolve this increasing difficulty.
Assessing the problem
If staff are to attempt to resolve aggression in the ED, it is necessary to assess and manage the problem from a holistic and caring viewpoint, maintaining the safety and dignity of everyone involved. The ED can appear a very hostile and threatening place to a patient or relative in an emotionally charged state. Brennan (1998), in examining the range of theories of aggression and violence, suggested that providing satisfactory definitions or an explanation as to where or how these behaviours originate is a complex task.
From a psychological perspective the occurrence of a sudden crisis resulting from a serious illness or accident, with the hurried removal of an individual to an ED, can often trigger strong emotions (Hildegard et al. 1987). These emotions of fear, anxiety, confusion and loss of control often result in stress reactions within the patient or relative and can be displayed in a variety of ways, sometimes displayed as aggression. Many individuals view the ED as an anxiety-provoking and hostile environment. In these situations adrenaline (epinephrine) is released, and the classical ‘flight or fight’ response triggered. Freud (1932) argued that aggression was an innate, independent, instinctive tendency in humans. In contrast, Bandura (1973) identified the way in which children learn aggressive responses by role modelling what they had observed in adults. Bateson (1980) further argued that an individual is only aggressive when assessed in relation to the other people or surroundings affecting that individual. Dollard et al. (1939) suggested the hydraulic type model of aggression where he viewed the need to release built-up frustration as a natural event similar to that of a pressure cooker effect. The frustration of prolonged waiting times in ED can also trigger an aggression (Derlet & Richards 2000), however Crilly et al. (2004) found that 67% of patients who exhibited violent behaviour had been in the departments for less than 1 hour.
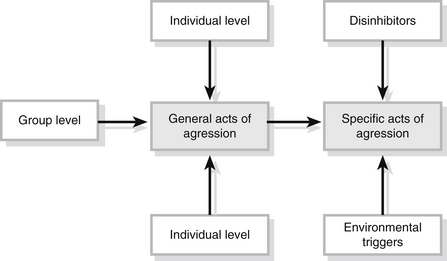
In reviewing the theories underpinning the development of aggression, Brewer (2007) identified a synthesis model of aggression within which the individual’s general level of aggression is determined by the combination of three types of factors; the individual, group and social (Fig. 12.1). In this model, physiological factors and neurochemical changes in the individual may combine with perceptions of other people’s behaviour to influence their response to an event or a situation. In this interpretation of factors that influence a person’s aggressive response, family or peer group views of acceptable levels of aggression or violence may also influence the individual’s response. Finally, this model acknowledges the impact of social factors such as the frequency of aggression portrayed on televions and the acceptability by society.
The major contribution made by physiological factors in the development of aggression in the ED has been identified as being the high consumption or withdrawal from alcohol or drugs (Jenkins et al. 1998). Intoxication with these drugs not only reduces the individual’s capacity to understand and interpret events, but also reduces inhibitory responses in times of stress. Violent incidents in the ED are more likely to occur within the hours of 00.00–07.00 with alcohol being identified as a major cause of violent behaviour (Schnieden & Marren-Bell 1995, Jenkins et al. 1998). Other organic reactions seen in acute confused states, e.g., metabolic disorders (diabetes or hypoxia resulting from respiratory or head injuries) or pain, may result in altered perceptions for the patient. These alterations in perception may also result in a confused aggressive patient arriving in the ED. When admitting these patients, the nurse may have to utilize very well-developed communication skills in order to make themself understood. In this condition the patient also may experience major problems in perceiving what is happening.
From an organizational viewpoint, the location of the ED, e.g., near to the public street, and 24-hour access may also attract a number of hostile individuals (Lyneham 2000). Distressed or psychologically disturbed patients often attend ED aware of the immediate access to medical and nursing care for crisis intervention. Their confused or distressed state may also result in aggressive responses to the ED staff. The ED itself can also influence the level of aggression displayed by patients and relatives who attend. The frustration that results from unrealistic expectations of the service may produce conflict and confrontation between the nurse and the patient or relative. Brewer (2007) suggests that the negative perceptions of the NHS often portrayed in the media may also impact upon the level of aggression demonstrated towards NHS staff. Lack of information and long waiting times for treatment as a result of poor staffing levels can also lead to frustration and anger (Jenkins et al. 1998). Poor waiting environments with lack of stimulation have also been suggested as being influential in developing aggression.
Further research suggests that less-experienced staff who demonstrated a more authoritarian attitude were potentially more at risk of assault (Breakwell & Rowett, 1989). Studies also identify that certain characteristics might be associated with some assaulted staff, which made them more prone to being assaulted (Lanza et al. 1991). The key element in all these studies is the nurse’s ability to communicate in a positive and caring manner with the patient or client. The importance of the nurse’s verbal and non-verbal communications with the patient or relative is demonstrated to be very important in conveying a caring, understanding attitude to an individual in times of stress or crisis, and in averting confrontation or aggression. It is acknowledged, however, that it may be difficult for the nurse to mask their underlying negative views on a patient and prevent negative non-verbal cues from being transmitted.
Identifying and recording the incidence of violence and aggression in the ED
Many authors suggest that aggressive incidents within healthcare and the ED are not recorded, and it is therefore difficult to measure the problem accurately (Forrester 2002, Pawlin 2008). This may be as a result of the lack of appropriate strategies and structures with which to recognize and record these incidents that occur all too regularly in ED. The Royal College of Nursing (2008) identifies a growing need for NHS staff to have access to the appropriate tools to identify the nature of the problem of violence and aggression in the workplace. They also recognize the lack of knowledge and information held by individuals, teams and organizations in relation to this issue, identifying a structure for risk assessments that should be undertaken to assess the problem. For staff, one of these risk assessments may require a review of the particular factors that influence aggression and violence in this particular environment, identifying practical measures within the emergency setting to address these factors.
Careful consideration of seating arrangements and decor of ED can help to reduce stress in those waiting to be treated. Other measures such as providing up-to-date reading material and a television or radio within the waiting area can reduce the boredom and frustration so often experienced while waiting in ED. The use of videos/DVDs explaining the organization of the ED or providing healthcare information can reduce tension and anxiety in the waiting area. These measures can also be employed to provide health promotion advice to the public. The provision of information is easily the most important issue to stressed relatives and friends, with other environmental factors also impacting on the level of anxiety and frustration experienced by the patient or relative (Box 12.1).
Box 12.1 Reducing the risk of violence
• All areas should look clean and welcoming, paying special attention to reception areas
• There should be adequate warmth and ventilation
• Noise should be minimized, e.g., by keeping the television volume at a comfortable level
• Designated separate smoking areas as appropriate
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


