2 Advanced Airway Techniques
 Key Points
Key Points• Advanced airway management is predicated on selecting the right technical approach for a given patient.
• Anticipated difficult airway management often relies on a sedated (or “awake”) technique.
• An organized approach (and backup plan) is essential for success with an unanticipated difficult airway.
Perspective
The cognitive skills to determine when a patient requires airway support are as important as the manual skills to accomplish the task. Currently, rapid-sequence intubation (RSI) is the most frequently used and successful means of intubating the trachea in emergency medical practice.1–4 It is clear that combining the use of a paralytic agent with a sedative agent has resulted in more successful laryngoscopy.5,6 This has led to fewer failed airways. Because every attempt at intubation may be difficult, a prepared and practiced backup or contingency plan is vital. The discussion of the various techniques and adjunctive measures that follows in this chapter reflects their application within an overall strategy.
In some cases the use of paralytics (i.e., RSI) is inappropriate because of a relatively high likelihood of intubation failure and subsequent worsening of the clinical condition linked to intubation attempts and the probability of failed ventilation. Accordingly, it is important to distinguish patients who are likely to be difficult to intubate, ventilate, and rescue (which often means performing a cricothyrotomy). These concepts are emphasized by the LEMON, MOANS, and SHORT mnemonics7 covered in Chapter 1. What follows is an overview of a strategic approach to advanced emergency airway management.
Epidemiology
A difficult airway (a case in which intubation is difficult to achieve) in the emergency department (ED) is far less studied but is probably experienced more frequently than in the more controlled environment of the operating suite. Patient extremis and lack of patient preparation make encountering both anticipated and unanticipated difficult airways more likely, with some estimates as high as 20%.8 Fortunately, however, the frequency of intubation failure in the ED is much lower and approximates 1%.3,9,10 The prevalence of airways requiring rescue from previous failed attempts in the ED is difficult to determine. What is apparent is that rescue devices are not used routinely, although they are commonly available.11,12
Anticipated Difficulty
Multiple predictors related to airway anatomy have been reported in the anesthesia literature, but none have been shown to be useful in isolation for predicting intubation difficulty.13–18 However, some evidence suggests the use of a limited set of assessments in patients undergoing airway management in the ED. The LEMON mnemonic has been proposed for this purpose19,20 (Box 2.1) (see Chapter 1). If difficulty is predictable and the patient is not a suitable candidate for RSI, the optimal approach depends on the previous training of the intubator and the availability of advanced airway tools.
Anticipated Difficult Airway
Only a small fraction of patients undergoing ED intubation are actually deemed poor candidates for RSI, even though many patients are expected to be difficult to intubate. No discreet threshold at which RSI is deemed to be safe and when it is contraindicated has ever been determined, partly because of the lack of sensitivity of the various difficult airway prediction tools. Importantly, many ED patients are in extremis and unable to cooperate with a preprocedural examination.21,22 Much of what is discussed in the current literature is based on the anesthesia experience, which generally reflects the “elective” intubation of cooperative patients. Nevertheless, it is often useful to perform a preprocedural assessment, as allowed by time constraints and the patient’s condition. Some evaluation is necessary to be able to accurately estimate the potential for encountering a difficult airway.
The algorithm presented in Figure 2.1 represents a clinical approach to a difficult airway.7 Application of such an approach is predicated on the answers to several key questions:
• Is there enough time to plan a methodic approach?
• Despite the identified presence of difficult airway predictors, can RSI still be used safely?
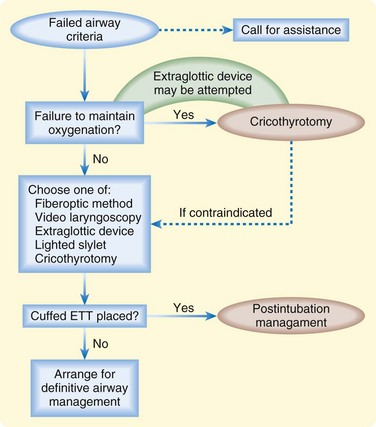
Fig. 2.1 Difficult airway algorithm.
(Adapted from Walls BM. The emergency airway algorithms. In: Walls RM, Murphy MF, editors. Manual of emergency airway management. 3rd ed. Philadelphia: Lippincott Williams & Wilkins; 2008.)
Optimized Laryngoscopy
Head and Neck Positioning
In the absence of cervical spine immobilization, active range of neck flexion and extension can frequently provide markedly improved visualization.23
External Laryngeal Manipulation
External manipulation of the larynx is distinct from the familiar cricoid pressure concept (e.g., the Sellick maneuver). It is, however, related to BURP (backward, upward, rightward pressure). The process of laryngeal manipulation is active. It requires that the intubator actively move the larynx to maximize visualization of the laryngeal structures. Generally, once the view is optimized, an assistant will be required to maintain the preferred positioning.24–26
Alternative Techniques for the Anticipated Difficult Airway
Fiberoptics
As a class, directable and flexible scopes have been available for decades. They have recently been made more portable by replacing the heavy light source with a battery pack. These devices are consequently more convenient in the harried ED. The majority of the products currently on the market consist of a directable cable mechanism associated with a light source and fiberoptic bundle. Notable issues are that the glass fibers that constitute the optics are breakable and small amounts of debris can greatly diminish viewing quality. Historically, these devices were considered too expensive or impractical. In the future, however, these type of flexible and directable devices will probably become more available. To date, relatively little research relevant to emergency medicine practice has been conducted.2,27–29 A recent query of emergency medicine training programs in the United States suggests that the majority maintain this type of equipment,11 but clinical expertise is variable.
Flexible and Directable Fiberoptics
Flexible and directable fiberoptic models are portable and have variable diameters and lengths. This equipment varies depending on its intended purpose. The shorter nasopharyngoscope is approximately 35 cm in length, in contrast to the 60-cm bronchoscope. The goal is to directly visualize the glottis via the nares or mouth. Once the cords are visualized, the tip of the fiberoptic scope is advanced into the airway to the level of the carina. The preloaded endotracheal tube is then advanced over the scope and into the airway. Efficacy of this technique in an awake patient requires adequate patient and equipment preparation (Box 2.2).
Box 2.2 Patient Preparation
If using a nasal approach, adequate topical anesthesia and vasoconstriction can be achieved with various agents via an atomizer.
If using an oral approach, various spray anesthetic agents can be used in addition to a nebulized agents (e.g., lidocaine). Additionally, gargled lidocaine (4%) can be effective, patient cooperation permitting.
An antisialagogue (e.g., glycopyrrolate) can be useful to allow better tissue absorption of topical anesthetic agents. However, at least 20 minutes is needed for efficacy as a drying agent.
Sedation is used, as necessary, to achieve reasonable anxiolysis to improve patient cooperation.
Preoxygenation, as always, is fundamental to procedural sedation and airway management.
Tips and Tricks
1. Recognize that the procedure will take at least 15 to 20 minutes to accomplish. If the patient cannot tolerate such a wait, use of this technique may be misguided.
2. Stay in the anatomic midline at all times during the procedure. Straying laterally will often result in poor visualization and inability to pass the vocal cords.
3. Keep the slack out of the scope. If slack is present along the length of the scope, rotation of the body of the scope will not translate into rotation of the tip.
4. The size of the working channel in many scopes is often too small for suction to be effective.
5. If the tube is resistant to passage of the scope into the airway, it is likely that the tip of the tube, or Murphy’s eye, is caught at the level of the arytenoids. Rotation of the entire tube-scope apparatus 45 to 90 degrees will probably overcome the obstruction.
Semirigid Fiberoptics
The semirigid fiberoptic scope is, conceptually, a semimalleable stylet with internal fiberoptic bundles.34 These devices are similar to the nondirectable class of fiberoptics with respect to image quality and durability. An example of this type of device is the Shikani optical stylet (Clarus Medical, LLC, Minneapolis, MN).
Rigid Fiberoptics
Rigid fiberoptic scopes consist of an imaging bundle enclosed within a rigid L– or J-shaped assembly. This shape is designed for placement into the hypopharynx with subsequent indirect visualization of the glottis. One of the chief advantages of these devices is that limited head, neck, and jaw mobility is less of a concern because of the ability to “look around the corner” of the hypopharynx. Examples in this class are the Bullard (Circon Corporation, Stanford, CT),35–37 WuScope Tubular Fiberoptic Laryngoscope (Achi Corporation, San Jose, CA),38–41 and UpsherScope (Mercury Medical, Inc., Clearwater, FL).42,43 These scopes are relatively expensive and their availability in the ED has been limited.11
Optical Laryngoscopy
Optical laryngoscopes use a series of lenses to provide a view of the anterior aspect of the glottis that is often not possible with direct laryngoscopy. Although image quality is inferior to that of video laryngoscopes, optical laryngoscopes are inexpensive, durable, and portable tools for difficult airway management. An example is the Airtraq, a disposable optical laryngoscope with a J-shaped blade that allows visualization of the glottis with the head and neck in a neutral position. In small randomized and nonrandomized studies, the Airtraq improved glottic exposure, reduced intubation difficulty scores, decreased cervical spine motion, and caused less change in the heart rate than did direct laryngoscopy with a Macintosh laryngoscope.44–46
Video Laryngoscopy
Video laryngoscopes use either a micro video camera or more traditional fiberoptic bundles encased in a laryngoscope handle design. Placement of the camera is meant to provide a wide-angle view of the glottis but is somewhat more removed from the various debris issues often encountered with the optics-in-the-tube format. The GlideScope (Verathon, Inc., Bothell, WA) is an example of the micro video camera design. This device is relatively new with limited ED experience.47 The literature that exists suggests that it can be used with very little motion of the cervical spine and that glottic visualization is generally excellent.48–51 However, actual intubation may be a bit more of a challenge because it requires an extreme “hockey stick” angulation of the styletted endotracheal tube to reach the glottis. Currently, laryngoscope sizes available correspond roughly to Macintosh No. 4 and No. 2, as well as pediatric sizes.

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


