ACUTE CHOLECYSTITIS
CASE SCENARIOS
 Case 1
Case 1
A 45-year-old obese woman presents to the emergency department with a 1-day history of constant right-sided abdominal pain. She has had similar episodes before; however, in prior instances the pain was self-limited and subsided within hours. She also reports nausea, vomiting, and low-grade fevers at home. Her medical history includes 4 prior cesarean sections.
On examination, she appears mildly uncomfortable with pulse of 85 beats per minute, blood pressure 140/95 mm Hg, and temperature of 100.8°F. Her abdomen is soft and nondistended, with focal right upper quadrant (RUQ) tenderness. Her labs reveal a white blood cell (WBC) count of 12,000, a total and direct bilirubin of 1.2 and 1.1, with an alkaline phosphatase (AP) of 98 and normal aspartate aminotransferase (AST) and alanine aminotransferase (ALT).
 Case 2
Case 2
The medical intensive care unit (ICU) team requests a consult for a 70-year-old man hospitalized for 2 weeks with pneumonia. He has been intubated and sedated since hospital day 2, is on 2 vasopressors, and has been on total parenteral nutrition (TPN) for 7 days. His medical history includes diabetes mellitus, hypertension, and chronic obstructive pulmonary disease. On physical examination, his abdomen is soft and mildly distended, and a mass is appreciable in the RUQ. He appears jaundiced. His most recent respiratory cultures have been negative, but he continues to have fevers to 101°F and a persistent leukocytosis, with a WBC ranging from 12,000 to 16,000. He also has mildly elevated liver function tests, with total bilirubin of 2.5, AP of 200, AST of 65, and ALT of 82.
 Case 3
Case 3
A 65-year-old man presents to the emergency department with a 2-day history of right-sided abdominal pain. He reports that the pain is constant and has gradually worsened. He is also complaining of nausea, vomiting, and fevers. His medical history is significant for diabetes mellitus and hypertension.
On examination, patient is ill appearing and is noted to have a temperature of 101.4°F, heart rate of 105 beats per minute, and blood pressure of 135/95 mm Hg. His abdominal examination is significant for RUQ tenderness to palpation with associated crepitus. Pertinent labs include a leukocytosis of 14,000/cc, elevated total bilirubin of 2.3 mg/dL, and indirect bilirubin of 1.7 mg/dL.
EPIDEMIOLOGY
Cholecystitis is one of the most common diagnoses encountered by general surgeons. In the United States, 10% to 15% of adults have gallstones, and 1% to 4% of these patients become symptomatic each year.1 Gallstones are either cholesterol or pigment based. Risk factors for developing cholesterol stones include female gender (especially women who have had multiple pregnancies), obesity, rapid weight loss, elevated serum triglyceride levels, Western diet (high fat and low fiber), and diabetes.2 Pigment stones tend to develop after prolonged fasting, TPN use, ileal resection, vagotomy, hemolytic states, cirrhosis, and bile duct stasis.2
Of patients with acute cholecystitis, 5% to 10% have acalculous cholecystitis, a condition that develops in approximately 0.2% to 0.4% of critically ill patients.3 Affected patients tend to be older (age 60 and above) and male, with a male-to-female ratio of 2–3:1.3 Acalculous cholecystitis usually has a more fulminant course than calculous cholecystitis, as the incidence of empyema, gangrene, or perforation is over 50%. It has a 40% mortality rate, primarily due to concurrent disease processes in the critically ill.2 It is most commonly seen in ICU patients following trauma, burns, prolonged TPN use, and major nonbiliary operations (Abdominal aortic aneurysm [AAA] repair, cardiopulmonary bypass).3
Emphysematous cholecystitis is rare and occurs in both calculous and acalculous cholecystitis. There is a high risk of gallbladder gangrene and perforation. The mortality rate is also high, approximately 15%, compared to the 3% to 4% mortality rate for acute cholecystitis without emphysema.4 It is more common in older patients (age 50–70), males, and diabetics.5 Approximately one-third of patients with emphysematous cholecystitis have diabetes.5,6
PATHOPHYSIOLOGY
Acute calculous cholecystitis occurs when gallstones occlude the cystic duct, leading to gallbladder distension and inflammation. Approximately 50% of patients have positive bile cultures, with Escherichia coli being the most common organism.2 Most gallstones are either cholesterol (70%–80%) or pigment (20%–30%) stones.2 Pathogenesis of cholesterol gallstones involves a combination of cholesterol supersaturation in bile and crystal nucleation, combined with gallbladder dysmotility, decreased gallbladder absorption, and increased secretion. Black pigment stones, meanwhile, are usually associated with hemolytic conditions or cirrhosis, and form when there is an increase in overall bilirubin or a higher concentration of unconjugated bilirubin. Brown pigment stones tend to occur in the bile ducts and are associated with biliary motility disorders and bacterial infection. Bacteria-producing slime and bacteria-containing glucuronidase, such as E. coli, Bacteroides, and Clostridium, cause enzymatic hydrolysis of conjugated bilirubin glucuronide to form free bilirubin, which precipitates with calcium to form stones.
The etiology of acalculous cholecystitis is unclear, but is likely related to a combination of gallbladder stasis and ischemia. Gallbladder stasis, caused by fasting, ileus, obstruction, or postsurgical irritation, can lead to bile inspissation, which is toxic to the gallbladder epithelium and can lead to colonization of the gallbladder with bacteria.3 Gallbladder ischemia, most commonly due to systemic inflammation from sepsis, leads to increased epithelial permeability and ultimately epithelial damage. Together, the epithelial damage and bacterial invasion culminate in acute cholecystitis.
Emphysematous cholecystitis occurs when gas-forming organisms infect the gallbladder. The most common bacteria involved are Clostridium perfringens, E. coli, Klebsiella spp, and anaerobic Streptococci. As with acalculous cholecystitis, the etiology of emphysematous cholecystitis is poorly understood. However, it likely arises from a combination of gallbladder ischemia and proliferation of gas-forming bacteria.
CLINICAL PRESENTATION
Patients with acute cholecystitis generally present with sustained RUQ pain and tenderness, fever, and leukocytosis. The duration of pain differentiates biliary colic, which is self-limited and usually lasts 4 to 6 hours, from acute cholecystitis, in which tenderness can persist for days. Patients often complain of referred pain to the right shoulder, back, or scapula. Nausea, emesis, anorexia, and fever are common, although not specific.
On physical examination, patients have localized RUQ tenderness and guarding and in classic cases have inspiratory arrest during deep palpation of the RUQ, called a “Murphy’s sign.” In one-third of patients, a RUQ mass may be palpated.2 Patients can also present with mild jaundice, although a total bilirubin >3 g/dL mandates workup for possible common bile duct obstruction. Laboratory values may reveal a mild leukocytosis (WBC 12,000–15,000) and mild elevations in alkaline phosphatase, AST, and ALT.2
Patients with acute acalculous cholecystitis present similarly to patients with acute calculous cholecystitis. Jaundice is more common, appearing in up to 20% of patients, as inflammation can extend into the common bile duct and cause partial biliary obstruction.7 Diagnosis can be difficult. Many patients are too ill to be able to describe symptoms, and other ongoing disease processes in critically ill patients may contribute to the observed abnormal laboratory values. In these cases, imaging can be extremely helpful in the diagnosis.
In emphysematous cholecystitis, RUQ pain, fever, nausea, vomiting, and leukocytosis are also seen. Rarely, crepitus is noted in the abdominal wall adjacent to the gallbladder. Patients can also have an unconjugated hyperbilirubinemia secondary to hemolysis caused by infection by Clostridium spp.
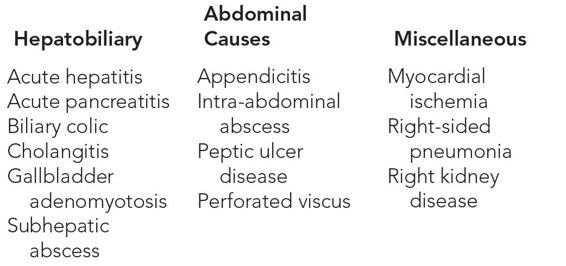
DIFFERENTIAL DIAGNOSIS
See Table 15–1.
WORKUP AND CHOICE OF IMAGING
Ultrasound is the imaging mode of choice for patients with cholecystitis. It is portable, noninvasive, fast, does not expose the patient to radiation, is more readily available, and has 81% sensitivity and 83% specificity.1 The ultrasound can also be useful in imaging the common bile duct.
CT scan is not the preferred mode of imaging for suspected cholecystitis because it is less sensitive than ultrasound, more expensive, and less accurate in its characterization of the common bile duct. The one exception is emphysematous cholecystitis, for which CT is highly sensitive. CT scan is also particularly helpful to detect other biliary pathology or intra-abdominal processes, such as pancreatitis or gallbladder cancer.
Radionuclide scans, also known as cholescintigraphy scan or hepatobiliary iminodiacetic acid (HIDA) scan, can be useful in atypical cases of acute cholecystitis. It is often used when there is high clinical suspicion for acute cholecystitis with a negative ultrasound. Both sensitivity and specificity can reach 95% for acute cholecystitis.2 False-positive HIDA results can occur with prolonged fasting (over 24–48 hours), severe hepatocellular disease, severe chronic acalculous cholecystitis, rapid biliary-to-bowel transit, and severe illness that leads to overall depressed physiology.3 The false-positive rate can be as high as 40%.2
Magnetic resonance cholangiopancreatography (MRCP) is another noninvasive technique that evaluates the biliary tract. It is especially useful in evaluating the intrahepatic and extrahepatic biliary systems. MRCP has a 90% sensitivity and 100% specificity for identifying stones in the biliary system and is often used to identify common duct stones.2 However, when compared to ultrasound, it is less sensitive for detecting signs of cholecystitis such as gallbladder wall thickening (sensitivity 69% vs 96%).8 Another disadvantage of MRCP is its high cost. Although its ability to detect biliary obstruction is comparable with endoscopic retrograde cholangiopancreatography (ERCP), some critics argue against using MRCP as it is an expensive test and can delay care as it does not allow for intervention.8
IMAGING FINDINGS
 Abdominal Ultrasound
Abdominal Ultrasound
Normal Gallbladder
On ultrasound, a normal gallbladder appears as a pear-shaped sac in the right upper quadrant. It is a hypoechoic structure with a smooth, uniform hyperechoic wall. The upper limit of normal for the gallbladder wall thickness is 3.5 cm. A normal gallbladder also does not contain stones and is not surrounded by fluid. Polyps under 1 cm are normal. Sonographic Murphy’s sign (focal tenderness over gallbladder using ultrasound probe) is absent (Figure 15–1).
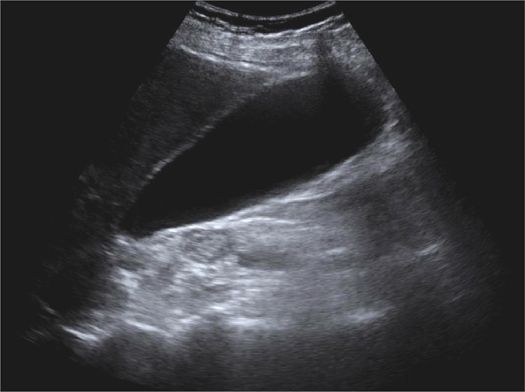
Figure 15–1 Normal gallbladder. The gallbladder wall is thin, uniform, and smooth. No sludge or stones are noted. There is no fluid surrounding the gallbladder.
Acute Cholecystitis
Findings suggestive of acute cholecystitis include gallbladder wall thickening (>3.5 mm), pericholecystic fluid, edema (double wall sign), and sonographic Murphy’s sign (Table 15–2 and Figure 15–2).







