Blunt trauma accounts for >90% of injuries in children.
8-12% of blunt trauma victims will have abdominal injuries.
Penetrating injuries account for less than 10% of all abdominal injuries.
Although more common than thoracic injuries, abdominal injuries are 40% less fatal.1
Mortality from solid organ injuries is typically determined by the degree of injury.2,3
PATHOPHYSIOLOGY
Motor vehicle crashes (MVCs), pedestrian collisions, and falls are the most common mechanisms of pediatric abdominal trauma.4
Be suspicious of possible abdominal injuries in seatbelt injuries, handlebar injuries, nonaccidental injuries, and snowboarding and all-terrain vehicle accidents.4
There are important anatomic differences between children and adults:
Children are smaller, transferring kinetic energy over a smaller area.4
Ribs are less calcified and more pliable, resulting in more force transmitted to thoracic and upper abdominal organs.4
Thinner abdominal wall and weaker musculature provide less protection to intra-abdominal organs.4
Infants and young children are at higher risk for multiple organ injuries due to the close proximity of intra-abdominal organs.4
INITIAL EVALUATION
See Chapter 2 on Primary and Secondary Survey for details.
Resuscitate by following Advanced Trauma Life Support (ATLS) guidelines.
Maintain a high index of suspicion for abdominal injuries in children.
Most solid organ abdominal injuries are treated nonoperatively.
Nonoperative treatment requires an accurate diagnosis and evaluation of injuries.
Decision to manage abdominal injuries nonoperatively should be reserved for centers experienced in this approach.
The appropriate expertise (surgical, critical care, anesthesia, nursing, and blood bank) is required to enable rapid operative treatment in case of complications.
HISTORY
Acquire an “AMPLE” history: Allergies, Medications, Past medical history, Last meal, and Events (mechanism).
Acquire a detailed history of the mechanism of injury.
Unclear mechanism or repeated visits to the emergency room should raise suspicion for nonaccidental injuries.
Certain traumatic mechanisms indicate patterns of injury.5 For example, handlebar, seatbelt, and nonaccidental injuries are associated with pancreatic and duodenal injuries.6,7
Children with bleeding disorders are at high risk from solid organ injuries even with minor injury mechanisms.4,8 and 9
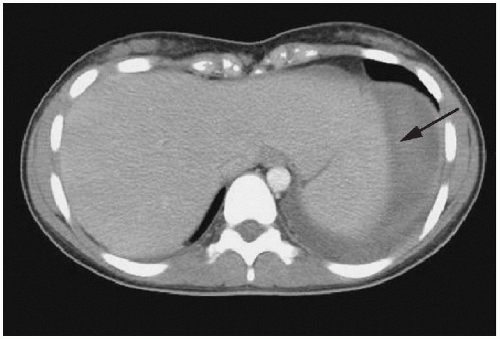
Epstein-Barr virus (EBV) infection with splenomegaly places children at high risk of splenic rupture from trivial trauma mechanisms (Fig. 11-1).4
FIGURE 11-1 • Adolescent female with mononucleosis presented with splenic rupture after a trivial fall. CT scan shows free fluid (arrow) in left upper quadrant.
PHYSICAL EXAMINATION
Physical signs indicative of possible abdominal injuries include:
Abdominal tenderness.
Distension.
Abrasions.
Ecchymosis.
Cotton and associates documented the predictive value of these physical examination abnormalities (tenderness Odds Ratio (OR) 40.7, ecchymosis OR 15.8, and abrasions OR 16.8).10
Accurately examining a small child with trauma can be challenging due to age, limited verbal ability, and distraction from painful injuries.11
Repeated physical examination improves accuracy and confidence.
Presence of the seatbelt sign (ecchymosis across the abdomen caused by wearing a lapbelt) should raise suspicion of intra-abdominal injuries (Fig. 11-2).
Due to aerophagia, abdominal distension in children is commonly from gastric distension (Fig. 11-3).
Early placement of nasogastric or orogastric tubes along with Foley catheterization allows for more accurate abdominal physical exam.
FIGURE 11-2 • Seatbelt sign. This patient has classic abdominal wall contusion and abrasions.
FIGURE 11-3 • Gastric distension. Significant abdominal distension in children may be caused by gastric distension from aerophagia.
LABORATORY INVESTIGATIONS
Laboratory tests in pediatric trauma should include:
Complete blood count (CBC).
Blood type and screen.
Serum electrolytes and glucose.
Venous blood gas and renal function.
Liver transaminases (ALT, AST).
Amylase and/or lipase.
Coagulation profile (INR, PTT).
Urinalysis (UA).
Beta-HCG (if a female is more than 10 years of age).
Toxicology screen as indicated.
Laboratory investigations are a screening tool for intra-abdominal injuries.
Their true utility is uncertain.
Results may suggest an injury and call for definitive imaging.
Amylase:
Often initially normal in pancreatic injuries.
Can be abnormal with no pancreatic injury.
Elevation may reflect:
Salivary amylase from head and neck injury.
Bowel obstruction.
Small bowel injury.
Elevated amylase <500 µ/L in the short-term should raise suspicion of hollow viscous injury.
Holmes and associates performed a prospective, nonrandomized study examining the utility of laboratory testing in pediatric abdominal trauma while adjusting for physical examination findings.12
1,095 injured children presented to an American level 1 trauma center.
107 of 1,095 (10%) had abdominal injuries.
Using a logistic regression model and internally validating the model, the independent predictors of abdominal injuries were found to be: Predictor OR (95% CI).
Low blood pressure, 4.1 (1.1, 15.2).
Abdominal tenderness, 5.8 (3.2, 10.4).
ALT >125 or AST >200, 17.4 (9.4, 32.1).
UA showing >5 RBC/hpf, 4.8 (2.7, 8.4).
IMAGING
Diagnosis of intra-abdominal injuries relies on diagnostic imaging modalities.
History, physical exam, and laboratory investigations are important screening tools for abdominal injuries but have limited sensitivity and specificity.
Radiologic modalities used are as follows:
X-Rays
Pediatric trauma patients should receive the standard:
Abdominal series have no role in investigating acutely injured children.
Computed Tomography (CT)
Intravenous contrast-enhanced CT is the gold standard for diagnosing and evaluating intra-abdominal injuries.
CT evaluates solid organs, hollow viscera, free air, and the retroperitoneum.
Hemodynamic stability is a prerequisite to acquiring a CT scan.
The need for oral contrast is controversial.
Proponents argue oral contrast may enhance diagnostic utility of CT in hollow viscus injuries.
Opponents of oral contrast stress:
The risks of vomiting and aspiration, especially in children with both torso and head injuries.
It does not have time to opacify the distal bowel, and therefore does not fully rule out a perforated viscus.
Delaying CT until full bowel opacification is achieved is unacceptable for trauma patients.
In a recent prospective adult study, 500 patients in a level 1 trauma center underwent IV contrast-enhanced CT without oral contrast:13
Sensitivity and specificity of CT for detecting blunt bowel injuries were 90.5 and 99.6, respectively.
At the Hospital for Sick Children, oral contrast is used selectively, reserving it for patients with a high pretest likelihood of having a duodenal injury.
To rapidly assess for free fluid in the abdomen or in the pericardial sac.
Widely accepted in the initial workup of adult trauma patients.
Created to replace diagnostic peritoneal lavage (DPL), not CT scan.
FAST is reliable in detecting abdominal free fluid in pediatric patients.5
Utility of FAST in children is questionable.
Hemoperitoneum alone is NOT an indication for surgery in children.
Almost all solid organ injuries (liver/spleen) are managed nonoperatively.
FAST may play a role in very specific clinical scenarios:
A hemodynamically unstable child who requires emergency surgery (e.g., craniotomy), to rule out the abdomen as the source of hemorrhagic shock.
To triage patients for CT scans of the abdomen, as 41% to 75% of scans performed for trauma are normal (e.g., FAST could act as a screening tool for the need for CT scan).
Maintenance of FAST skills can be challenging with low volumes of pediatric trauma.
Use of FAST in pediatric trauma should be determined on an institution-specific basis.
MRI
MRI is not needed for managing pediatric abdominal or pelvic trauma.
May be beneficial for certain disease processes.
GI Studies
UGI series, small bowel follow-through, and contrast enemas have no role in workup of an acutely injured child.
Diagnostic Peritoneal Lavage (DPL)
CT scan availability has eliminated need for DPL in traumatized children.
A positive DPL is NOT an indication for abdominal surgery in hemodynamically stable patients.
DPL provides no information about retroperitoneal injuries.
Performed by infusing 10 mL/kg normal saline into peritoneal cavity followed by gravity drainage of fluids and examination (gross and microscopic) of the fluids.