Chapter 8.2 Interdisciplinary management of chronic pelvic pain A US physical medicine perspective
Introduction
As discussed in Chapter 8.1, historically, medical management of chronic pelvic pain (CPP) has frustrated both patients and providers, leading to the evolution of multimodal therapeutic strategies. Specialists are now viewing CPP as a polymorphic syndrome that may include organic pathology, musculoskeletal dysfunction, neuropathology and psychosocial impairments. Medical practice utilizing interdisciplinary, co-ordinated interventions is resulting in more successful treatment outcomes (Montenegro 2008).
• In addition to genital, anal, coccygeal, perineal, buttock and abdominal pain, CPP can include urinary symptoms such as dysuria, urinary urgency, frequency, hesitancy and poor stream strength.
• Bowel complaints include constipation, difficulty with evacuation, dyschezia and ‘pencil stool’ or varied, abnormal shapes of stool.
• Sexually, patients may experience anorgasmia or difficulty achieving orgasm, genital hyperarousal disorder, post-orgasmic pain, pain during or after intercourse, erectile dysfunction and/or excessive or lack of vaginal discharge in women.
Due to the varied symptoms, patients may seek the help of primary care physicians, gynaecologists, urologists, colorectal surgeons, orthopedists, neurologists and/or psychiatrists. It is reported that 85–90% of patients with CPP have musculoskeletal dysfunction (Tu et al. 2006, Butrick 2009) that has been identified as either a primary cause of pain and dysfunction or a secondary consequence of vulvodynia, painful bladder syndrome/interstitial cystitis, chronic pelvic pain syndrome/non-bacterial chronic prostatitis, irritable bowel syndrome, pudendal neuralgia and endometriosis (Tu et al. 2006, Butrick 2009).
Furthermore, 30% of patients seen in primary care settings, and 85% in dedicated pain centres, are diagnosed with myofascial pain syndrome, demonstrating the importance of including musculoskeletal investigation early in the assessment of a patient with CPP (Butrick 2009). Ideally such investigation would be undertaken as part of a team approach to the condition.
Team management
As in the UK, physicians, physical therapists and mental health providers in the US commonly form interdisciplinary teams working with chronic pain in general and CPP in particular (see Figure 8.2.1). Surgical interventions and invasive procedures run the risk of symptom exacerbation in patients with CPP, therefore conservative therapies such as manual physical therapy techniques, psychotherapies and pharmaceuticals are often utilized first to modulate pain. Simultaneously, organic pathology needs to be addressed if identified. Interventional medicine strategies have shown efficacy in treatment of CPP and should be utilized if conservative measures fail (Simons et al. 1999, Zhang et al. 2004, Maria et al. 2005, Amir et al. 2006). Numerous treatment options exist, and more than one medical professional may be able to treat particular pathophysiological features, whereas certain treatments may only be available from one team member. Treatment of CPP should be considered as a dynamic process with many possible effective treatment combinations. Certain treatments will be more or less important than others as a patient’s presentation changes.
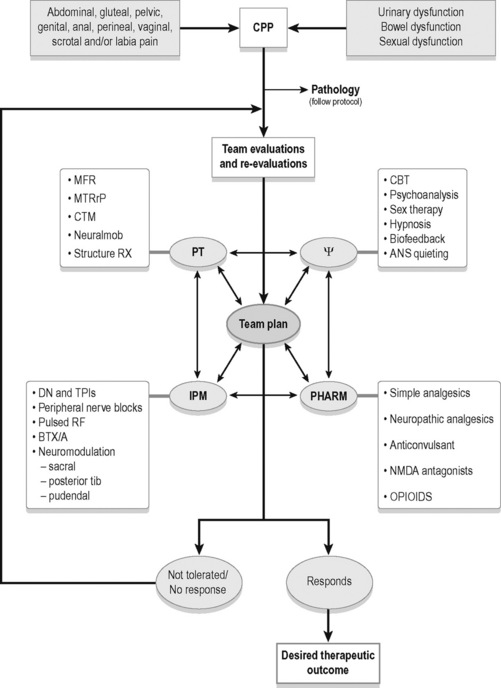
As CPP is a syndrome associated with numerous pathophysiological features (see Box 8.2.1), extensive patient education and excellent interdisciplinary communication is imperative. Commonly, the treatment of a single impairment does not translate into the dramatic change the patient may expect. For example, if a patient with a 5-year history of severe vaginal burning is given an anticonvulsant and the pain is reduced, but not eradicated, the patient reports ‘disappointment’, and may think ‘it is not working’. In actuality, studies cited later in this chapter show anticonvulsants are effective for treating the central processing dysfunction this patient likely has. However, this patient may also present with pelvic floor myofascial trigger points and pudendal nerve inflammation, and until these impairments are also addressed, the overall syndrome is likely to persist. Through examinations, re-examinations, differential diagnoses and communication, the team can manage patient expectations more effectively.
The interventions listed in this text are effective treatments for the pathophysiological features listed in Box 8.2.1. The multimodal algorithm (see Figure 8.2.1) helps explain how to turn the complex problem of CPP into a sum of more manageable parts, expanding on the decision-making process to determine when and how to use different modalities. Clinical examples will be used to demonstrate the utility of the interdisciplinary approach.
Organic pathology intervention
Organic pathologies associated with CPP may include: yeast and bacterial infections, urinary tract, bladder and prostate infections, irritable bowel syndrome, endometriosis, colitis, Crohn’s disease, gastritis and sexually transmitted diseases. Symptoms of these pathologies mimic the symptoms of CPP and appropriate treatment protocols for the pathology should be followed (Butrick 2009).
Cognitive behavioural therapy
Cognitive behavioural therapy (CBT) should be considered an important component in a comprehensive treatment plan for patients with CPP. Behavioural interventions for chronic pain have become commonly available alternatives to medical and rehabilitative therapies (Campbell & Mitchell 1996, Gatchel & Turk 1996). CBT has been shown to be an effective treatment for chronic pain patients, by helping to develop self-management skills to improve their personal control of their condition, reduce pain, distress, and pain behaviour, and improve daily functioning (Turk et al. 1983, Eccleston et al. 2009). Treatment that focuses on decreasing negative thinking, emotional responses to pain, and perceptions of disability, while increasing orientation toward self-management, are predictive of favourable treatment outcomes (Morely et al. 1999, McCracken & Turk 2002).
CBT has been shown to be efficacious for the treatment of vulvodynia in two uncontrolled studies (Abramov et al. 1994, Weijmar et al. 1996) and in one well-controlled, randomized study (Bergeron et al. 2008). Masheb et al. conducted a randomized trial to test the relative efficacy of CBT and supportive psychotherapy (SPT) in women with vulvodynia. The results suggest that psychosocial treatments for vulvodynia are well tolerated and produce clinically meaningful improvements in pain. They observed that CBT, relative to SPT, resulted in significantly greater improvements in pain severity and sexual function. Additionally, participants in the CBT condition reported significantly greater treatment improvement, satisfaction and credibility than in the SPT condition (Masheb et al. 2009).
Manual physical therapy intervention
The musculoskeletal impairments that may cause pelvic pain and dysfunction are connective tissue restrictions, muscle hypertonus with or without myofascial trigger points (including muscles of the pelvic floor, trunk and lower extremities), altered neurodynamics of peripheral nerves and pelvic girdle and biomechanical abnormalities. After a thorough history, an extensive physical examination is performed. The entire surface areas of the abdomen, trunk, thighs, pelvis (up to the base of the clitoris and penis including the labia and scrotum) should be examined for connective tissue restrictions (Fitzgerald 2009).
Conservative medical management starts with manual therapy to eradicate or modify the impairments, which may in turn, decrease pain. In 2009, the Urological Pelvic Pain Collaborative Research Network (UPPCRN) concluded that somatic abnormalities, including myofascial trigger points and connective tissue restrictions, were found to be very common in women and men with IC/PBS and chronic prostatitis/chronic pelvic pain syndrome, respectively (Fitzgerald et al. 2009).
Somatic abnormalities may be the primary abnormality in at least some patients and secondary in others, but in either situation they should be identified and treated. The UPPCRN also published the outcomes of their feasibility trial comparing connective tissue manipulation (CTM) and myofascial physical therapy, versus global therapeutic massage, in patients with CPP. The group receiving skilled CTM and myofascial therapy had a significantly higher response rate than the group receiving massage alone (Fitzgerald et al. 2009). See Chapter 11.2 for a summary of CTM methodology.
Altered neurodynamics
Compromised blood supply and/or neurobiomechanics of peripheral nerves may cause altered neurodynamics, thereby contributing to pelvic pain and dysfunction (Butler 2004). Connective tissue restrictions, muscle hypertonus and faulty joint mechanics can affect the dynamic protective mechanisms of peripheral nerves and lead to burning, stabbing, shooting pain in the territory of the nerve (Butler 2004).
For example, consider a patient with severe pelvic floor hypertonus. This patient may have inflammation around the pudendal nerve, secondary to compression by the muscles. Each time this patient attempts to have a bowel movement he is forced to strain, and several attempts are made before he succeeds at evacuating the stool. In addition to static compression causing inflammation, the muscles can fixate a normally mobile nerve as the patient forcefully lengthens the pelvic floor during straining. This can cause further neural irritation. The patient may experience shooting, stabbing rectal pain, either during or after the bowel movement, reflective of this neural irritation (Prendergast & Rummer 2008).
Treatment of altered neurodynamics involves removing the aggravating stimuli and restoring mobility. Myofascial treatment of connective tissue restrictions and muscle hypertonus may reduce aggravating neural input. Neural mobilization techniques to restore mobility along the path of the nerve have also shown efficacy (Ellis & Hing 2008).
Chapters 2, 9, 11, 12, 13 and 14 discuss the evaluation and treatment of the pelvic floor muscles, myofascial trigger points, biomechanics and the pelvic girdle at length.
Lifestyle modifications and home exercise programmes
All members of the interdisciplinary team can help the patient make temporary lifestyle modifications to improve function while the patient is being treated. Techniques to promote autonomic nervous system quieting, improve sleep hygiene, decrease stress, and improve diet and nutrition are all helpful, if not imperative, to the treatment process. Examples include the use of cushions, posture and/or breathing education, workstation, home and car modifications, clothing and footwear recommendations, and advice on exercise programme development (Prendergast & Rummer 2008).
Pharmacological therapy
The approach to pharmacological therapy for CPP in the USA is very similar to that in the UK. See Chapter 8.1.
Simple analgesics
Acetaminophen has both analgesic and antipyretic activity and has been used in acute and chronic painful conditions (Bannwarth & Pehourcq 2003); however, there is little evidence about its role in CPP. There is also very little evidence for the use of non-steroidal anti-inflammatory drugs (NSAIDs) in the treatment of CPP and even less for cyclo-oxygenase 2 (COX-2) selective drugs.
Neuropathic analgesics
Tricylic antidepressants are widely used for other chronic pain conditions such as fibromyalgia, chronic headaches, interstitial cystitis and irritable bowel syndrome. They have been studied for several pain disorders and have consistently shown benefit (Ohghena & Van Houdenhove 1992). The benefit of tricyclics is not generated by decreasing depression. If depression is present, it should be treated separately. Amitriptyline is the most commonly studied and has been shown to be an effective treatment for neuropathic pain, but side effects often limit its clinical use (Max 1994, Richeimer et al. 1997). A few studies have compared the use of amitriptyline versus placebo in patients with pelvic pain (McKay 1993). Some authors recommend it as the treatment of choice, whereas others have reported disappointing results (Richeimer et al. 1997, Rose & Kam 2002). Mixed reuptake inhibitors have been shown to be more effective than selective serotonin reuptake inhibitors in the treatment of chronic pain (Fishbain et al. 2000, Yokogawa et al. 2002).
Anticonvulsants
Anticonvulsants have been used in pain management for many years. Gabapentin has been reported to be well tolerated and an effective treatment in various pain conditions, particularly in neuropathic pain (Beydoun et al. 1995, Rosenberg et al. 1997). Gabapentin failed to show effectiveness in genitourinary tract pain in some studies, but has shown success in the treatment of diabetic neuropathy, post-herpetic neuropathy, neuropathic pain associated with carcinoma, multiple sclerosis, genitourinary tract pain and vulvodynia in others (Ben & Friedman 1999, Sasaki et al. 2001). Sator-Katzenschlager et al. reported that after 6, 12 and 24 months, pain relief was significantly greater in patients receiving gabapentin either alone or in combination with amitriptyline than in patients on amitriptyline alone. In this study gabapentin was more effective than amitriptyline in improving neuropathic burning or spontaneous, paroxysmal pain (Sator-Katzenschlager et al. 2005). Pregabalin (Lyrica) is a relatively new drug that has been found to be very beneficial for patients with myofascial pain disorder and neuropathic symptoms, such as in fibromyalgia (Butrick 2009).
N-methyl-D-aspartate antagonists
The N-methyl-D-aspartate (NMDA) receptor channel complex is known to be an important channel for the development and maintenance of chronic pain. NMDA antagonists have been useful in the management of neuropathic pain (Hewitt 2000). Ketamine has been beneficial in several chronic pain conditions including peripheral neuropathies, but its long-term role remains unclear (Visser & Schug 2006). Challenging pelvic pain conditions may be helped by ketamine if there is nerve injury or central sensitization.
Opioids
Opioids have a role in the management of chronic non-malignant pain, however, opioids in pelvic pain are poorly defined (McQuay 1999). The following guidelines for the use of opioids in chronic/non-acute urogenitial pain are (Fall et al. 2008):
• All other treatments must have been tried and failed;
• An appropriately trained specialist should consult with another physician when instigating opioid therapy;
• With a history or suspicion of drug abuse, psychological consultation is imperative;
• Patient should undergo a trial of opioids;
• Patient should be made aware of the rules and regulations of opioid use as well as the risk of addiction and dependency;
• Morphine is the first-line drug, unless there are contraindications to morphine or special indications for another drug.
Trigger point injection therapy
As described in Chapters 11 and 15, myofascial trigger points (MTrPs) are a nodular and hyperirritable area within a taut band of skeletal muscle. They can cause characteristic referred pain, local tenderness, autonomic phenomena, motor dysfunction and/or weakness and proprioceptive disturbances (Simons et al. 1999). Trigger points can be successfully treated with several approaches, one of which is trigger point injections. The most accepted theory hypothesizes that the mechanical disruption of the skeletal muscle fibres by an anaesthetic injection inactivates the trigger point (Simons 1999
Related posts:
 Psychophysiology and pelvic pain
Psychophysiology and pelvic pain
 Electrotherapy and hydrotherapy in chronic pelvic pain
Electrotherapy and hydrotherapy in chronic pelvic pain
 Biofeedback in the diagnosis and treatment of chronic essential pelvic pain disorders
Biofeedback in the diagnosis and treatment of chronic essential pelvic pain disorders
 Intramuscular manual therapy: Dry needling
Intramuscular manual therapy: Dry needling
 Patients with pelvic girdle pain: An osteopathic perspective
Patients with pelvic girdle pain: An osteopathic perspective
 Practical anatomy, examination, palpation and manual therapy release techniques for the pelvic floor
Practical anatomy, examination, palpation and manual therapy release techniques for the pelvic floor
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


