Edited by Anne-Maree Kelly Graeme Thomson Dysphagia is a broad term encompassing the many forms of difficulty with deglutition (swallowing). The main issues are to determine the likely cause, to identify those patients at risk of significant complications, to treat those causes that are amenable to acute intervention and to refer appropriately for further investigations and treatment. Dysphagia may be associated with odynophagia (pain on swallowing). Globus is a related term that means the sensation of a lump in the throat. This is rarely of psychological origin. Since the advent of sophisticated investigative techniques, it has been recognized that, in the great majority of cases, there is an identifiable physical cause. Problems may occur with any of the three stages of swallowing: oral, pharyngeal or oesophageal. Oral and pharyngeal causes may be grouped as transfer dysphagia and oesophageal problems may be referred to as transport dysphagia. Passage of food may be obstructed by a physical barrier, such as a tumour, or a disorder of muscle coordination, such as a neurological deficit. In addition to diseases, several drugs are recognized as inducing dysphagia. They include tetracyclines, non-steroidal anti-inflammatory drugs, ascorbic acid, quinidine, ferrous sulphate and potassium chloride. Symptoms may appear suddenly or develop insidiously. If insidious, there may be an acute precipitating event leading to presentation, often complete or partial obstruction owing to the impaction of a food bolus in the oesophagus. This may present as pain, a feeling of a lump in the neck or central chest, severe retching or drooling and an inability to swallow saliva. Patients may report increasing difficulty swallowing solids and then fluids but, in some cases, there may be no previous history of dysphagia. Where a neurological disorder is causing difficulty initiating swallowing, there may be other neurological deficits. The voice may have changed. Regurgitation of food from the mouth or nose, coughing or frank aspiration may be evident when the patient eats. It should be assumed that patients with recent cerebrovascular events or bulbar dysfunction have dysphagia until formal assessment of swallowing and airway protection can be undertaken. Examination should focus on testing cranial nerve function plus careful examination of the mouth, neck, chest and abdomen. Hydration status and nutritional status should be evaluated. Perforation may be suspected if there is a history of ingestion of a corrosive substance or sharp object or if pain is a prominent feature. There may be evidence of surgical emphysema in the neck. If presentation is delayed there may be signs of sepsis. Investigations are directed by the history and likely aetiology. For oropharyngeal and upper oesophageal lesions, a lateral X-ray of the soft tissues of the neck may reveal a lesion impinging on the oesophagus. An impacted dense bone or other solid foreign body may also be seen. For suspected mid- and lower-oesophageal lesions, frontal and lateral chest radiographs may reveal a fluid level, a mediastinal tumour, tuberculous lesions or an aneurysm of the thoracic aorta. Oesophageal perforation may also be detected. If food bolus obstruction is suspected a Gastrografin swallow may reveal the site and degree of obstruction. Computed tomography (CT) scanning and endoscopy may also be indicated but, in most cases, they can be deferred and performed on a semi-elective basis. A video-fluorographic swallowing study is the best semi-elective investigation. It may reveal structural abnormalities as well as disorders of muscular coordination. Manometry is less reliable. Laboratory investigations are guided by likely aetiology and complications, but should include basic biochemistry and full blood examination looking for electrolyte disturbances and anaemia. Definitive treatment depends on the underlying cause and will rarely be completed in the emergency department (ED). The degree of oesophageal obstruction, the acuity of onset and the presence of complications dictate the need for emergency treatment. Patients with high-grade obstruction should have oral fluids and food withheld and should be given intravenous fluids if the obstruction persists for more than a few hours. For food bolus obstruction, intravenous glucagon may relax the oesophageal muscles enough to allow a bolus to pass through. This is less likely to be successful if the bolus is a piece of meat. An initial dose of 1 mg may be followed by a 2 mg dose if necessary. Complications are rare, but include allergy, nausea and hypotension. Phaeochromocytoma is a contraindication to the use of glucagon. Sublingual glyceryl trinitrate may be used as an alternative to glucagon, but hypotension is more likely. After glucagon, a gas-producing substance may be given in an attempt to dilate the oesophagus. Aerated drinks are adequate for this purpose. This technique should be used with great caution because a patient with upper oesophageal obstruction will be at greater risk of aspiration if given a foaming substance. This approach should be avoided if there is any suspicion of perforation. Endoscopic removal will be required in many cases, but this is usually attempted after a period of expectant treatment. Bones or similar foreign bodies impacted in the pharynx can often be removed in the ED. Topical anaesthetic sprays may suppress the pharyngeal reflexes adequately to allow direct or indirect laryngoscopy and removal with forceps. Removal may immediately relieve the dysphagia, but symptoms due to local oedema or abrasions may persist. Oesophageal or pharyngeal perforation is a serious complication requiring cover with broad-spectrum antibiotics and urgent surgical referral. Odynophagia may be relieved by parenteral or topical analgesia. Oral administration of a viscous preparation of lignocaine will ease the pain caused by luminal inflammatory disorders. The maximum recommended dose is 300 mg and should be reduced in the elderly, who may be more affected by systemic absorption. If a patient with known chronic dysphagia presents to the emergency department for an unrelated reason, care should be taken to avoid giving food or fluids that may be aspirated. Water is associated with a high aspiration risk. Appropriate disposition depends on the likely aetiology and the presence of complications. Admission is indicated for patients at risk of airway compromise, severe haemorrhage, sepsis or those with high-grade oesophageal obstruction. It will also be indicated when dysphagia is part of a broader disease process. If a food bolus has passed spontaneously, the patient should be referred for semi-elective endoscopy. Kim Chai Chan and Eillyne Seow The assessment of patients with abdominal pain is challenging because: The emergency department (ED) approach to acute abdominal pain emphasizes disposition over diagnosis. It is more important to recognize an acute abdomen than to identify the exact cause of the pain. It has been estimated that abdominal pain accounts for approximately 5–10% of all ED visits. A significant proportion (18–42%) of these patients will require admission. The elderly (aged 60 and over) are over-represented in the admitted patient group. In one study of elderly patients presenting with abdominal pain, at least 50% were hospitalized and about 30–40% eventually required surgery. Up to 40% of patients were initially misdiagnosed and the overall mortality was about 10%. Abdominal pain may result from: Both visceral and somatic pain may manifest as referred pain. Some examples are: Table 7.2.1 Differential diagnosis of pain by location (list is not exhaustive) Generalized diffuse pain that is poorly localized may be due to benign causes (e.g. gastroenteritis, constipation and menstrual cramps) or from life-threatening conditions (Table 7.2.2). Table 7.2.2 Some potentially life-threatening causes of generalized, diffuse abdominal pain Haemoperitoneum from any cause, e.g. ruptured abdominal aortic aneurysm, ruptured ectopic pregnancy, trauma Mesenteric ischaemia Perforated viscus Peritonitis (any cause) Pancreatitis Bowel obstruction Diverticulitis Inflammatory bowel disease Metabolic disorders (e.g. diabetic ketoacidosis), sickle cell crisis, typhoid fever Adapted from Gray-Eurom K, Deitte L. Imaging in the adult patient with non-traumatic abdominal pain. Emerg Med Pract 2007;9:2 with permission. There are a number of extra-abdominal causes for abdominal pain that must be considered along with abdominal causes (Table 7.2.3). Table 7.2.3 Extra-abdominal causes of abdominal pain Thoracic Myocardial infarction/unstable angina Pneumonia Pulmonary embolism Herniated thoracic disc (neuralgia) Genitourinary Testicular torsion Systemic Diabetic ketoacidosis Alcoholic ketoacidosis Uraemia Sickle cell disease Systemic lupus erythematosus Vasculitis Hyperthyroidism Porphyria Glaucoma Toxic Methanol poisoning Heavy metal poisoning Scorpion bite Black widow spider bite Abdominal wall Muscle spasm Muscle haematoma Herpes zoster Infections Strep pharyngitis (more often in children) Mononucleosis Adapted from Purcell TB. Nonsurgical and extraperitoneal causes of abdominal pain. Emerg Med Clin N Am 1989;7:721 with permission. During triage, a rapid assessment is made by looking at the patient’s general condition as well as vital signs. Obviously ill patients, those in severe pain or with abnormal vital signs should be given priority. However, it is not possible to rule out life-threatening causes of abdominal pain by the absence of abnormal vital signs. It has been estimated that up to 7% of patients with normal vital signs may have an underlying life-threatening process and this percentage increases in the elderly. Tachycardia may be absent in patients with autonomic dysfunction, in the elderly and in patients on medications that may blunt the cardiac response to illness or volume loss. Similarly, the elderly, the immunocompromised or those in severe septic shock may sometimes not mount a febrile response. Even in the immunocompetent, fever may not always accompany acute inflammatory conditions. An accurate, focused history often provides the best clue to the possible aetiology of abdominal pain. Clinical impression derived from the history will direct decisions regarding further diagnostic work-up. Table 7.2.4 Common causes of abdominal pain according to age group and gender The nature and time course of pain are key clues to diagnosis. The following attributes should be noted: Table 7.2.5 Temporal characteristics of abdominal pain Sudden maximal pain at or near onset Perforated peptic ulcer Ruptured abdominal aortic aneurysm Ruptured ectopic pregnancy, ruptured ovarian cyst Ovarian/testicular torsion Mesenteric infarction Pulmonary embolism Acute myocardial infarction Progression to maximal pain within minutes Acute pancreatitis Renal and ureteric colic Biliary colic Strangulated hernia Volvulus Intussusception Gradual onset (increased pain over hours) Appendicitis Strangulated hernia Inflammatory bowel disease Chronic pancreatitis Salpingitis/prostatitis Cystitis From White MJ, Counselman FL. 2005 Troubleshooting acute abdominal pain. Emedmag 2002. http://www.emedmag.com/html/pre/cov/covers/011502.asp with permission. Patients with abdominal pain often have other associated symptoms that may give a clue to the possible cause. These include: Table 7.2.6 lists some of the historical high-yield questions in abdominal pain. Table 7.2.6 High-yield historical questions 1. How old are you? 2. Which came first – pain or vomiting? 3. How long have you had the pain? 4. Have you ever had abdominal surgery? 5. Is the pain constant or intermittent? 6. Have you had this before? 7. Do you have a history of cancer, diverticulosis, pancreatitis, kidney failure, gallstones, or inflammatory bowel disease? 8. Do you have human immunodeficiency virus (HIV)? 9. How much alcohol do you drink per day? 10. Are you pregnant? 11. Are you taking antibiotics or steroids? 12. Did the pain start centrally and migrate to the right lower quadrant? 13. Do you have a history of vascular or heart disease, hypertension or atrial fibrillation? Adapted from Colucciello SA, Lukens TW, Morgan DL. Assessing abdominal pain in adults: a rational, cost-effective, and evidence-based strategy. Emerg Med Pract 1999;1:1 with permission. A systematic, directed and thorough physical examination can help strengthen the clinical impression formed from the history or to uncover unexpected abnormalities. Physical findings help to rule in, but not rule out, the underlying diagnosis. Consider the general condition and the vital signs of the patient. Patients who look drowsy or unwell or have abnormal vital signs need urgent attention. The posture of the patient may give a clue to the possible underlying disease. Patients with renal colic typically roll about in pain, whereas those with peritonitis lie still as movements aggravate the pain. Inspect for pallor, jaundice, hydration status, enlarged lymph nodes and signs of chronic liver or renal disease. This is carried out with the patient lying supine and the abdomen exposed from the costal margins to the pubic symphysis. Ideally, the patient should be fairly relaxed, comfortable and cooperative. It is almost impossible to perform an abdominal examination in an uncooperative patient thrashing about in pain. Adequate pain relief should be given before examination if necessary. There is strong evidence that analgesia does not mask physical signs. Abdominal examination in an obtunded patient is unreliable and other assessment modalities such as imaging have to be considered. Table 7.2.7 From White MJ, Counselman FL. Troubleshooting acute abdominal pain Emedmag, 2005. http://www.emedmag.com/html/pre/cov/covers/011502.asp with permission. This is useful in cases of gastrointestinal haemorrhage, perianal or perirectal diseases, stool impaction, prostatic pathologies and rectal foreign bodies. Contrary to classic teaching, rectal examination does not provide additional input in suspected cases of appendicitis. All hernias should be examined for signs of strangulation. Hernias are most commonly present in the inguinal or femoral area, along the midline or arising from old surgical scars. Rarely, they may be present in the paramedian, lumbar or gluteal areas. In women, examination of the pelvic organs may yield important clues to possible gynaecological or obstetric causes of abdominal pain. Testicular pathology needs to be considered in male patients with lower abdominal pain. A significant proportion of patients with serious intra-abdominal conditions, such as ruptured aortic abdominal aneurysm and mesenteric ischaemia, may present with non-specific abdominal findings. The area of tenderness does not always correlate to the anatomical location of the disease. For example, up to 20% of patients with surgically proven appendicitis have no right lower quadrant tenderness. Signs of peritonism may not always be present, especially in the elderly and the immunocompromised. Although involuntary guarding or rigidity increase the likelihood of peritonitis, rebound tenderness has been shown to have no predictive value. Besides the abdomen, extra-abdominal systems, especially the cardiovascular and respiratory systems, should also be examined. Directed examination of extra-abdominal systems is important because: Physical signs may often be non-specific in the early phases of the disease. Serial examinations over a period of hours can help to distinguish a surgical from a non-surgical abdomen and improve the diagnostic yield. Although the history and physical examination may give a clue to the possible underlying pathology, many patients with abdominal pain do not present ‘classically’. Where indicated, judicious use of investigations may assist in determining diagnosis and disposition. An investigation should be ordered to answer focused clinical questions. It is also important to be aware of the test’s accuracy and limitations. Results should be interpreted in the correct clinical context. Negative test results may not fully rule out serious pathologies in patients with high pre-test probabilities. Further observation, reassessment and admission may need to be considered. Most laboratory tests do not aid in differentiating surgical from non-surgical causes of abdominal pain. The value of plain radiographs in the evaluation of patients with abdominal pain is limited. However, there is still a place for plain X-rays as a first-line investigation in patients with suspected bowel obstruction, bowel perforation and foreign body. A three-view series comprising upright chest, supine and upright abdominal radiographs is recommended. X-ray findings for bowel obstruction and perforation are fairly specific but not sensitive, i.e. they help to establish, but not exclude, these diagnoses. Ultrasound does not involve ionizing radiation, is rapid, non-invasive and may be performed at the bedside. This makes it the ideal evaluation tool in unstable patients or those who are pregnant. Selective use of focused ultrasound in the appropriate clinical context maximizes its diagnostic sensitivity. However, ultrasound is operator dependent and appropriate training is necessary to ensure competence. The sensitivity of ultrasound may also be reduced by technical limitations (e.g. obesity, bowel gas, subcutaneous emphysema). Focused bedside emergency ultrasound examination has significantly affected the diagnosis and management of the following life-threatening conditions: Ultrasound may also be used for evaluating patients in the following conditions that may not be immediately life threatening: With the advent of helical and multidetector scanning technology, CT has become the imaging modality of choice for evaluation of abdominal pain in the non-obstetric patient. It has a high degree of accuracy, establishing diagnoses in more than 95% of cases in one study. In the elderly, CT resulted in changes to the management and disposition of a significant proportion of patients. CT allows for detailed visualization of intra-, extra- and retroperitoneal structures. It identifies the exact site of disease, as well as its impact on the surrounding structures, thereby guiding further management. CT may be performed with or without intravenous and oral contrast agents. In the emergency setting, CT is useful for: The main limitations to CT are that the patient must be stable enough for transport to the scanning facility, ionizing radiation is involved, it may miss up to 20% of gallstones because the stones may be of the same radiographic density as bile and it may miss up to 10–17% of traumatic small bowel perforations. The sensitivity of CT is not 100% for most conditions. Clinical decisions should not be based on CT results alone. If initial CT findings are negative but clinical suspicion is high, further observation, evaluation or even repeat scans may be needed. In the patient with very high suspicion for conditions that require immediate surgical intervention (e.g. unstable patient with obvious peritonitis), use of CT may result in delay in definitive treatment. For the patient in whom the clinical suspicion for serious abdominal pathology is very low, urgent CT scan is likely to have a low yield and the cost and potential side effects of CT outweigh its benefits. In one study for ED patients with suspected urgent abdominal conditions, a diagnostic strategy with initial ultrasound examination, followed by CT when ultrasound findings were negative or inconclusive, resulted in the best CT sensitivity. This strategy also reduced CT use by up to 51%. With the introduction of high-speed techniques, MRI protocols for patients with acute abdominal pain can now be reduced to below 15 minutes. MRI does not involve ionizing radiation and offers better soft tissue visualization than CT. The high intrinsic contrast resolution of images rendered by MRI may allow for contrast-free scanning in certain cases. Compared to CT, MRI is able to provide increased information for hepatobiliary disease, pancreatitis and mesenteric ischaemia. MRI has also demonstrated promising accuracy for diagnosis of appendicitis, diverticulitis, small bowel obstruction and abdominal and pelvic venous thrombosis. Currently, the evidence for use of MRI in ED patients presenting with acute abdominal pain is still relatively limited; it is most frequently used in selected pregnant patients in whom ultrasound findings are non-diagnostic. MRI is significantly more costly than CT, takes longer to perform and may have limited availability in some centres. MRI is contraindicated in patients with claustrophobia or implanted metallic devices. Ultrasound is currently still the most common initial imaging modality used to evaluate the pregnant patient presenting with acute abdominal pain, although MRI is now playing an increasingly important role. Both imaging techniques do not involve ionizing radiation and have not been shown to cause any ill effects to the fetus. The routine use of gadolinium-based MR contrast agents is currently not recommended as these agents pass through the placenta into fetal circulation and their effects on the fetus remain unknown. CT is a valuable imaging tool in evaluation of abdominal pain in the pregnant patient, as it remains one of the most reliable imaging modality in the diagnoses of many acute abdominal conditions. The ionizing radiation doses involved in CT studies are below the doses that would lead to developmental or neurological deficits. However, radiation levels should still be kept as low as reasonably achievable as there are no known radiation limits for fetal stochastic effects, e.g. carcinogenesis. Iodine-based CT contrast agents are also known to cross the placenta into fetal circulation. Small studies have indicated that single dose exposure to CT contrast agents does not lead to fetal teratogenesis or hypothyroidism. Similar to MR contrast agents, intravenous CT contrast agents should be avoided unless the accuracy of the imaging study is dependent on their use. In elderly patients presenting with abdominal pain, conditions requiring surgical intervention (e.g. cholangitis, intestinal obstruction), serious vascular pathologies (e.g. AAA, aortic dissection, mesenteric ischaemia) and intra-abdominal neoplasms are more common (Table 7.2.8). Unfortunately, abdominal pain is frequently misdiagnosed in the elderly because: Table 7.2.8 Disease spectrum in those less than 50 years old vs those over 50 Adapted from deDombal FT. Acute abdominal pain in the elderly. J Clin Gastroenterol 1994;29:331–5 with permission. Adverse outcomes in the elderly are more common as a result of missed or delayed diagnosis than in younger patients. This is because the elderly tend to seek treatment late in the disease process and complications tend to be more common, they have reduced physiological reserve and often more co-morbidities. It has been estimated that with each decade of life, diagnostic accuracy decreases while mortality increases, such that for the octogenarian diagnostic accuracy is about 30%, although the corresponding mortality rate is 70 times that of patients under 30. Therefore, geriatric patients with abdominal pain need to be carefully evaluated and the threshold for imaging studies, surgical consultation and admission should be lowered. Inflammatory responses are suppressed in the immunocompromised and abdominal signs from peritoneal irritation may be absent. Patients with human immunodeficiency virus (HIV) infection may develop unusual conditions, such as opportunistic viral or bacterial enterocolitis (e.g. cytomegalovirus or Mycobacterium avium intrecellulare enterocolitis), AIDS-related cholangiopathy, lymphoma or drug-induced pancreatitis. Patients on peritoneal dialysis or with advanced liver cirrhosis are at risk of developing spontaneous bacterial peritonitis. It is important to determine whether these patients are pregnant. Menstrual history, compliance with contraception, history of tubal ligation or claims of sexual abstinence cannot reliably exclude the possibility of pregnancy. If the patient is pregnant, the possibility of ectopic pregnancy should be considered. In addition, pelvic conditions (e.g. pelvic inflammatory disease, ovarian pathology, pregnancy-related complications, such as threatened or missed abortion) and urinary tract infections are relatively common. For patients in the second or third trimester of pregnancy, the gravid uterus may displace structures in the lower abdomen away from their usual position, e.g. the appendix may migrate to a higher position in the right hypochondrium or the right flank, changing symptoms and signs. Clinical signs of peritonism may be obscured due to loss of abdominal wall musculature elasticity. Misdiagnosed patients are most commonly given the labels of gastroenteritis, constipation, gastritis, urinary tract infection or pelvic inflammatory disease. Table 7.2.9 From Colucciello SA, Lukens TW, Morgan DL. Assessing abdominal pain in adults: a rational, cost-effective, and evidence-based strategy. Emerg Med Pract 1999;1:1 with permission. In the ED management of patients presenting with abdominal pain, empirical management of acute conditions and proper disposition are more important than diagnostic accuracy. When the diagnosis is based only on clinical findings and basic laboratory investigations, overall diagnostic accuracy is about 50% (as high as 80% in young adults and as low as 30% in the elderly). Fortunately, the rate of inappropriate discharge from the ED is low (about 1% across all age groups), albeit slightly higher in the elderly (about 4%). Prompt resuscitation should take precedence over diagnosis in unstable patients. Patients may be in shock as a result of blood loss, fluid loss, sepsis or from concurrent cardiovascular events. Appropriate fluid therapy and inotropic support should be instituted early to prevent further deterioration and end-organ dysfunction. Pain relief should be instituted as early as possible for patients presenting with abdominal pain. This may require intravenous opiates titrated to response. Specific treatment (e.g. non-steroidal anti-inflammatory agents in renal colic) should be used when available. The previously widely held dogma that opiates mask signs of serious pathology (in particular peritonism) has been disproved in many studies. In fact, the use of opioids in abdominal pain is not only safe, but actually aids diagnosis by facilitating physical examination and relaxing the abdominal musculature. The dosage used should be titrated to the patient’s response. Antibiotics are indicated in suspected intra-abdominal sepsis. The antibiotics used should cover Gram-negative aerobes as well as anaerobes. Additional coverage for Gram-positive aerobes is required in patients with spontaneous bacterial peritonitis. See chapters on specific conditions for more details. Early involvement of surgeons should be the rule in cases of suspected surgical abdomen. Early surgical intervention is crucial in improving outcome for urgent conditions, e.g. ruptured abdominal aortic aneurysm, ruptured ectopic pregnancy, intraperitoneal haemorrhage and bowel perforation. The following patients need to be admitted: In addition, the admission threshold should be lowered for patients returning to the ED for the same complaints, especially where the cause of the abdominal pain had not been fully elucidated. Patients who do not meet admission criteria but have persistent pain may be observed over a period of hours, in the ED or an observation unit if appropriate. Serial examination over a period of hours has been found to improve diagnostic accuracy. The main aims of observing the patient with abdominal pain are to improve diagnostic yield with serial examination, to monitor progress after treatment, to detect the development of signs of acute abdomen and for further diagnostic work-up if indicated. It is important to give discharge advice, as some conditions develop over time. The patient should be advised to return if:
Digestive Emergencies
7.1 Dysphagia
Introduction
Aetiology
Clinical features
Clinical investigations
Treatment
Disposition
7.2 Approach to abdominal pain
Introduction
 the degree of pain may not be commensurate with the severity of the disease
the degree of pain may not be commensurate with the severity of the disease
 the absence of abnormal vital signs cannot rule out a serious underlying condition
the absence of abnormal vital signs cannot rule out a serious underlying condition
 a large number of potential differential diagnoses may need to be considered.
a large number of potential differential diagnoses may need to be considered.
Epidemiology, pathophysiology and differential diagnosis
 Visceral pain: this pain is poorly localized and may be colicky, intermittent and recurrent in nature. Stimulation of nociceptors investing the visceral peritoneum causes visceral pain. For example, when hollow organs are distended or when capsules covering solid organs are stretched. Visceral pain localizes to the abdominal region that correlates with the embryonic segments of the viscera:
Visceral pain: this pain is poorly localized and may be colicky, intermittent and recurrent in nature. Stimulation of nociceptors investing the visceral peritoneum causes visceral pain. For example, when hollow organs are distended or when capsules covering solid organs are stretched. Visceral pain localizes to the abdominal region that correlates with the embryonic segments of the viscera:
 foregut structures (stomach, duodenum, liver, biliary tract, pancreas) localize to the upper abdomen
foregut structures (stomach, duodenum, liver, biliary tract, pancreas) localize to the upper abdomen
 midgut structures (small bowel, proximal colon, appendix) localize to the periumbilical region and
midgut structures (small bowel, proximal colon, appendix) localize to the periumbilical region and
 hindgut structures (distal colon, genitourinary tract) localize to the lower abdomen.
hindgut structures (distal colon, genitourinary tract) localize to the lower abdomen.
 Somatic pain: this pain is well localized and is often constant and intense. Somatic pain results from local irritation of the parietal peritoneum. It is localized more specifically to the area of pathology. Differential diagnosis of pain by location is shown in Table 7.2.1. It is, however, important to recognize that the area of pain does not always correspond to the supposed anatomical location of the underlying pathology, e.g. acute appendicitis may present as suprapubic or flank pain.
Somatic pain: this pain is well localized and is often constant and intense. Somatic pain results from local irritation of the parietal peritoneum. It is localized more specifically to the area of pathology. Differential diagnosis of pain by location is shown in Table 7.2.1. It is, however, important to recognize that the area of pain does not always correspond to the supposed anatomical location of the underlying pathology, e.g. acute appendicitis may present as suprapubic or flank pain.
 shoulder pain due to diaphragmatic irritation
shoulder pain due to diaphragmatic irritation
 pain at the tip of the scapula due to gallbladder pathology
pain at the tip of the scapula due to gallbladder pathology
Right upper quadrant
Epigastrium
Left upper quadrant
Right lumbar or flank
Midline or periumbilical
Left lumbar or flank
Right lower quadrant
Suprapubic
Left lower quadrant
Pain radiating to the back
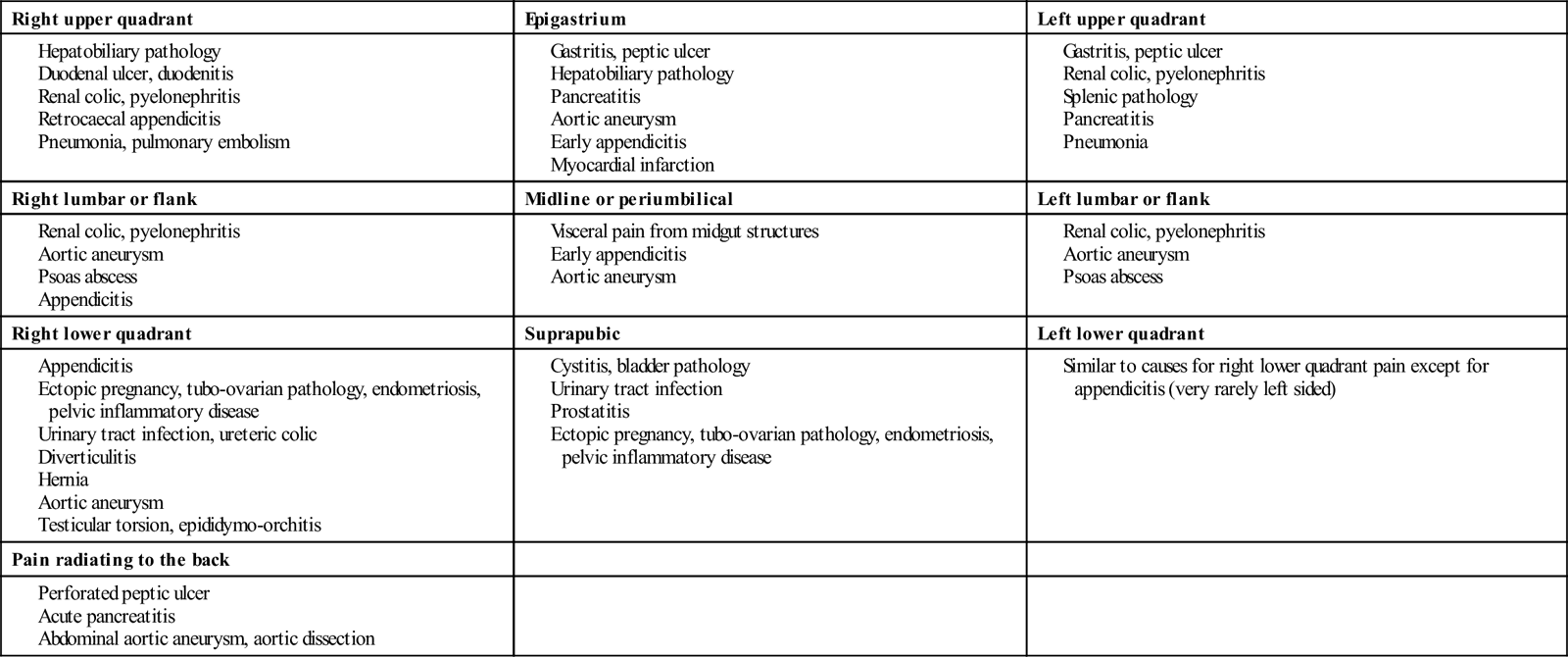
Causes of diffuse abdominal pain
Extra-abdominal causes of abdominal pain
Clinical features
Vital signs and general condition
History
Patient demographics and background history
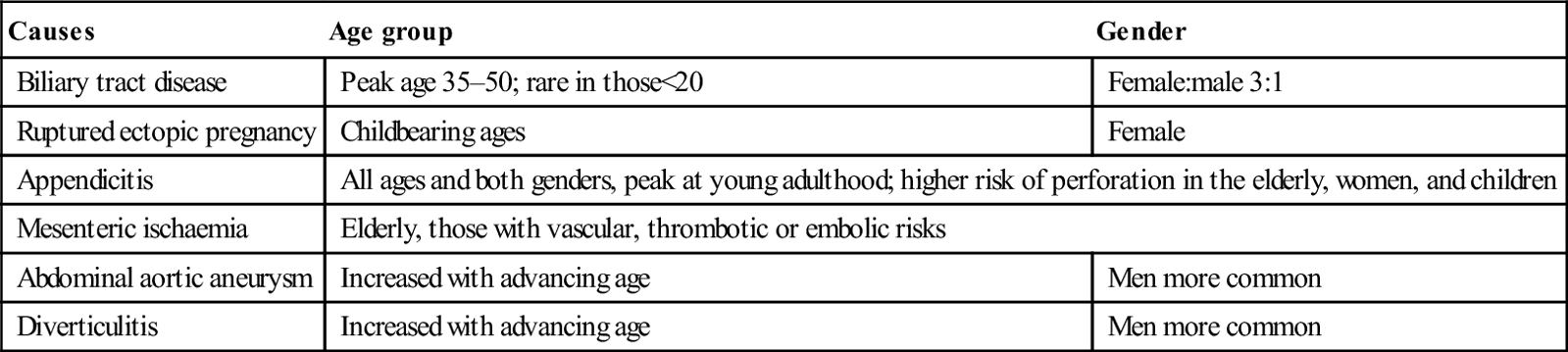
 Age and gender: the likelihood of certain conditions is higher in patients of a specific age and gender (Table 7.2.4). For women of childbearing age, it is important to ascertain the presence or absence of pregnancy.
Age and gender: the likelihood of certain conditions is higher in patients of a specific age and gender (Table 7.2.4). For women of childbearing age, it is important to ascertain the presence or absence of pregnancy.
 Background history: key questions in the background history are:
Background history: key questions in the background history are:
 use of tobacco, alcohol or recreational drugs
use of tobacco, alcohol or recreational drugs
Causes
Age group
Gender
Biliary tract disease
Peak age 35–50; rare in those<20
Female:male 3:1
Ruptured ectopic pregnancy
Childbearing ages
Female
Appendicitis
All ages and both genders, peak at young adulthood; higher risk of perforation in the elderly, women, and children
Mesenteric ischaemia
Elderly, those with vascular, thrombotic or embolic risks
Abdominal aortic aneurysm
Increased with advancing age
Men more common
Diverticulitis
Increased with advancing age
Men more common
Pain attributes
 Onset and progress of abdominal pain over time (Table 7.2.5): acute vascular events and rupture of hollow viscus typically presents with maximal pain at the onset. Ureteric and biliary colic also often presents with severe pain in the early stages. This is in contrast to pain from inflammatory processes, such as acute appendicitis, which tends to progress and ‘mature’ over hours.
Onset and progress of abdominal pain over time (Table 7.2.5): acute vascular events and rupture of hollow viscus typically presents with maximal pain at the onset. Ureteric and biliary colic also often presents with severe pain in the early stages. This is in contrast to pain from inflammatory processes, such as acute appendicitis, which tends to progress and ‘mature’ over hours.
 Location of pain (see Table 7.2.1), migration of pain, radiation of pain: location of pain helps to identify the area of pathology, although occasionally this may be misleading, especially if the pain is referred. Migration of pain over time gives a clue to possible underlying aetiology, e.g. pain from appendicitis typically starts at the umbilicus or epigastrium and later localizes to the right iliac fossa.
Location of pain (see Table 7.2.1), migration of pain, radiation of pain: location of pain helps to identify the area of pathology, although occasionally this may be misleading, especially if the pain is referred. Migration of pain over time gives a clue to possible underlying aetiology, e.g. pain from appendicitis typically starts at the umbilicus or epigastrium and later localizes to the right iliac fossa.
 Radiation of pain may suggest specific conditions (see Table 7.2.1), e.g. pain from acute pancreatitis and perforated peptic ulcers often radiates to the back.
Radiation of pain may suggest specific conditions (see Table 7.2.1), e.g. pain from acute pancreatitis and perforated peptic ulcers often radiates to the back.
Associated symptoms
Advanced age means increased risk
Pain first is more likely to be caused by surgical disease
Pain for less than 48 hours is more likely to be caused by surgical disease
Consider adhesion or obstruction in patients with previous abdominal surgery
Constant pain is more likely to be caused by surgical disease
A report of no prior episode is more likely to be caused by surgical disease
All are suggestive of more serious disease
Consider occult infection or drug-related pancreatitis
Consider pancreatitis, hepatitis, cirrhosis
Test for pregnancy; consider ectopic pregnancy
These may mask infection
High specificity for appendicitis
Consider mesenteric ischaemia and abdominal aneurysm
Physical examination
General
The abdomen
 Specific abdominal signs (Table 7.2.7): distinctive signs have been described that are associated with specific diagnoses. Some of these signs have not been studied and their sensitivity and specificity remain unknown.
Specific abdominal signs (Table 7.2.7): distinctive signs have been described that are associated with specific diagnoses. Some of these signs have not been studied and their sensitivity and specificity remain unknown.
Sign
Description
Association
Murphy’s sign
Inability of patient to perform deep inspiration due to pain on palpation of right hypochondrium
Acute cholecystitis (sensitivity 97%; specificity 50%)
Kehr’s sign
Severe left shoulder tip pain, especially when the patient is lying supine
Haemoperitoneum, e.g. from ruptured spleen or ectopic pregnancy
Cullen’s sign
Ecchymoses around the periumbilical area
Retroperitoneal haemorrhage (haemorrhagic pancreatitis, abdominal aortic aneurysm rupture)
Grey–Turner’s sign
Ecchymoses of the flanks
Retroperitoneal haemorrhage (haemorrhagic pancreatitis, abdominal aortic aneurysm rupture)
McBurney’s sign
Tenderness localized to a point at two-thirds distance on a line drawn from the umbilicus to the right anterior superior iliac spine
Appendicitis
Iliopsoas sign
Extension of right hip causes abdominal pain
Appendicitis (sensitivity 16%; specificity 95%)
Obturator’s sign
Internal rotation of the flexed right hip causes abdominal pain
Appendicitis
Rovsing’s sign
Right lower quadrant (RLQ) pain with palpation of the left lower quadrant
Appendicitis
Heel-drop sign
RLQ pain on dropping heels on the ground after standing tiptoes; alternatively RLQ pain from forcefully banging the patient’s heel with the examiner’s hand
Appendicitis (sensitivity 93%)
Cough test
Post-tussive abdominal pain
Peritonitis (sensitivity up to 95%)
Rectal examination
Examination of hernia orifices
Examination of genitalia
Limitations of the abdominal examination
Examination of extra-abdominal systems
Serial examination
Clinical investigations
Bedside tests
Laboratory tests
Imaging
Plain X-rays
Ultrasound
Computed tomography
 assessment in abdominal trauma
assessment in abdominal trauma
 detection of inflammatory lesions (e.g. appendicitis, pancreatitis, diverticulitis, abscesses)
detection of inflammatory lesions (e.g. appendicitis, pancreatitis, diverticulitis, abscesses)
 detection of neoplastic lesions
detection of neoplastic lesions
 evaluation of vascular pathology (e.g. aortic aneurysm, aortic dissection, mesenteric ischaemia)
evaluation of vascular pathology (e.g. aortic aneurysm, aortic dissection, mesenteric ischaemia)
 detection of intra-abdominal and retroperitoneal bleed or abscesses
detection of intra-abdominal and retroperitoneal bleed or abscesses
Magnetic resonance imaging (MRI)
Imaging for the pregnant patient
Pitfalls
The elderly
 pain perception in the elderly may be blunted
pain perception in the elderly may be blunted
 vital signs may be normal in spite of serious underlying illness
vital signs may be normal in spite of serious underlying illness
Confirmed cause of acute abdominal pain
Acute abdominal pain in patient<50 (n=6317) (%)
Acute abdominal pain in patient≥50 (n=2406) (%)
Biliary tract disease
6
21
Non-specific abdominal pain
40
16
Appendicitis
32
15
Bowel obstruction
2
12
Pancreatitis
2
7
Diverticular disease
<0.1
6
Cancer
<0.1
4
Hernia
<0.1
3
Vascular
<0.1
2
The immunocompromised
Women of childbearing age
Dangerous mimics (Table 7.2.9)
True diagnosis
Initial misdiagnosis
Appendicitis
Gastroenteritis, pelvic inflammatory disease (PID), urinary tract infection (UTI)
Ruptured abdominal aortic aneurysm
Renal colic, diverticulitis, lumbar strain
Ectopic pregnancy
PID, UTI, corpus luteum cyst
Diverticulitis
Constipation, gastroenteritis, non-specific abdominal pain
Perforated viscus
Peptic ulcer disease, pancreatitis, non-specific abdominal pain
Bowel obstruction
Constipation, gastroenteritis, non-specific abdominal pain
Mesenteric ischaemia
Constipation, gastroenteritis, ileus, small bowel obstruction
Incarcerated or strangulated hernia
Ileus, small bowel obstruction
Shock or sepsis from perforation, bleed and abdominal infection in the elderly
Urosepsis or pneumonia (in elderly)
Diagnosis versus disposition
Treatment
Resuscitation
Symptom relief
Antibiotics
Surgical review
Disposition
Admission
 patients with specific diagnoses that require inpatient management
patients with specific diagnoses that require inpatient management
 patients who are ill, unstable or with altered mentation
patients who are ill, unstable or with altered mentation
 the elderly or the immunocompromised in whom diagnoses are unclear
the elderly or the immunocompromised in whom diagnoses are unclear
 patients in whom potentially serious conditions cannot be excluded
patients in whom potentially serious conditions cannot be excluded
 patients in whom symptoms (e.g. pain, vomiting) cannot be ameliorated
patients in whom symptoms (e.g. pain, vomiting) cannot be ameliorated
 patients who are unable to follow discharge instructions or who have poor social support.
patients who are unable to follow discharge instructions or who have poor social support.
Observation
Discharge advice
 pain is persistent (>24 hours) or worsening
pain is persistent (>24 hours) or worsening
 they develop incessant vomiting or are unable to retain fluids
they develop incessant vomiting or are unable to retain fluids
 vague pain has become localized, e.g. to the right iliac fossa
vague pain has become localized, e.g. to the right iliac fossa
 they develop high fever or chills, or feel increasingly ill, weak or unwell
they develop high fever or chills, or feel increasingly ill, weak or unwell
 they develop fainting episodes
they develop fainting episodes
 there is blood in the stools or vomitus
there is blood in the stools or vomitus
 they develop new medical problems requiring urgent consultation.
they develop new medical problems requiring urgent consultation.Related posts:
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree

















































