Edited by Anne-Maree Kelly Weng Hoe Ho and Ken Ooi The upper respiratory tract extends from the mouth and nose to the carina. It comprises a relatively small area anatomically, but is of vital importance. The majority of presentations are not life threatening, however, those that are require immediate evaluation or treatment. Emergent conditions are those likely to compromise the airway. Protection and maintenance of airway, breathing and circulation (the ABCs) take precedence over history taking, detailed examination or investigations. Possible causes of airway obstruction are listed in Table 6.1.1. Table 6.1.1 Causes of upper airway obstruction Altered conscious state Head injury Cerebrovascular accident Drugs and toxins Metabolic – hypoglycaemia, hyponatraemia, etc. Foreign bodies Infections Tonsillitis Peritonsillar abscess (quinsy) Epiglottitis Ludwig’s angina Other abscesses and infections Trauma Blunt or penetrating trauma resulting in oedema or haematoma formation Uncontrolled haemorrhage Thermal injuries Inhalation burns Neoplasms Larynx, trachea, thyroid Allergic reactions Anaphylaxis Angioedema Anatomical Tracheomalacia – congenital or acquired (secondary to prolonged intubation) Other congenital malformations Acute on chronic causes Patients with chronic narrowing of the airway (e.g. due to tracheomalacia) may present worsening obstruction with an acute upper respiratory tract illness or injury Non-urgent presentations include rash or facial swelling not involving the airway, sore throat in a non-toxic patient and complaints that have been present for days or weeks with no recent deterioration. Pharyngitis and tonsillitis are common causes for presentation in both paediatric and adult emergency practice. Initial evaluation should be aimed at differentiating those patients needing urgent management to prevent significant morbidity and mortality from those needing less urgent treatment. Triage must be based on the chief complaint and on vital signs since the same clinical presentation may result from a range of pathologies. For example, stridor can be due to trauma, infection, drug reactions or anatomical abnormalities, such as tracheomalacia. Symptoms and signs of airway obstruction include dyspnoea, stridor, altered voice, dysphonia and dysphagia. Evidence of increased work of breathing includes subcostal, intercostal and suprasternal retraction, flaring of the nasal alar as well as exhaustion and altered mental state. The presence of these signs may vary with age and accompanying conditions. Cyanosis is a late sign. Further examination will be directed by the presenting complaint and initial findings and includes: Upper-airway obstruction may be acute and life threatening or may have a more gradual onset. It is essential that the adequacy of the airway is assessed first. Any emergency interventions that are required to maintain the airway should be instituted before obtaining a detailed history and examination. This may range from relieving the obstruction to providing an alternative airway. Obstruction may be physiological with the patient unable to maintain and protect an adequate airway due to a decreased conscious state. Despite the plethora of possible causes, the initial treatment of securing the airway is the same regardless of the cause. Mechanical obstruction may be due to pathology within the lumen (aspirated foreign body), in the wall (angio-oedema, tracheomalacia) or by extrinsic compression (Ludwig’s angina, haematoma, external burns). Obstruction may be due to a combination of physiological and mechanical causes. A summary of potential causes of upper airway obstruction is provided in Table 6.1.1. Investigations are secondary to the assessment of and/or provision of an adequate airway. Once the airway has been assessed as secure, the choice of investigations is directed by the history and examination. Direct laryngoscopy by an experienced operator is the single most important manoeuvre in patients with acute upper airway obstruction. It may concurrently form part of the assessment, investigation or treatment. By visualizing the laryngopharynx and upper larynx, the cause of the obstruction can be seen. Any foreign bodies may be removed or, if necessary, a definitive airway, such as an endotracheal tube, introduced. In the case of the stable patient with an incomplete obstruction, this should only be attempted when there are full facilities available for intubation and provision of a surgical airway. It may be more appropriately deferred until expert airway assistance is available. Bronchoscopy may be required to assess the trachea and distal upper airway but it is not part of the initial resuscitation. In the stable patient, it is more appropriate to transfer the patient to the operating suite or ICU for this procedure. Some blood tests may be useful in guiding further management. These include full blood count, arterial blood gases and blood cultures. Those required will be guided by the clinical presentation. Initial treatment in the emergency department should not await their results. A lateral soft tissue X-ray of the neck is sometimes helpful once the patient has been stabilized. Metallic or bony foreign bodies, food boluses or soft tissue masses may be seen. A number of subtle radiological signs have been described for epiglottitis (Table 6.1.2). Table 6.1.2 Radiological findings in adult epiglottitis In the patient with a mechanical obstruction, a computed tomography (CT) scan of the neck and upper thorax may be helpful in diagnosing the cause of the obstruction as well as the extent of any local involvement. It may aid in planning further management, especially if surgical intervention is indicated, for example for a retrothyroid goitre or head and neck neoplasm. Management initially consists of securing the airway. This is discussed in more detail elsewhere in this book, but simple interventions include chin lift or jaw thrust and an oropharyngeal airway. More sophisticated procedures, such as the laryngeal mask or endotracheal tube insertion or surgical airway, may be required. A surgical airway is rarely necessary in the emergency department, although it is important that equipment is available and that the techniques have been practised. These include needle insufflation and cricothyrostomy. A number of commercial kits, such as the Mini-trach II and the Melker Emergency Cricothyroidotomy Catheter Set, are available. Further management will depend on the underlying cause. Further treatment will be dictated by the underlying pathology. Foreign body aspiration is often associated with an altered conscious state, for example in alcohol or drug intoxication, cerebrovascular accident (CVA) or dementia. Elderly patients with dentures are at increased risk. Laryngeal foreign bodies are almost always symptomatic and are more likely to cause complete obstruction than foreign bodies below the epiglottis. Foreign bodies in the oesophagus are an uncommon cause of airway obstruction but, if lodged in the area of the cricoid cartilage or the tracheal bifurcation, they can compress the airway causing partial airway obstruction. Oesophageal foreign bodies may also become dislodged into the upper airway. In the management of incomplete airway obstruction with adequate gas exchange, care should be taken not to convert partial obstruction into complete obstruction by overzealous intervention. Awake laryngoscopy can be performed to visualize the foreign body and remove it. The management of complete airway obstruction depends on the conscious level of the patient. In conscious patients, the Heimlich manoeuvre (or abdominal thrust) is one recommended technique for dislodgement of a foreign body. The rescuer stands behind the patient placing clenched fists over the patient’s upper abdomen well clear of the xiphisternum. A short sharp upward thrust is made to force the diaphragm up and expel the foreign body. There is a risk of injury to internal organs and thus should only be done by rescuers who have been trained in the technique. Chest thrusts may be more effective in obese patients if the rescuer is unable to encircle the patient’s abdomen. Chest thrusts may also be used in children or in pregnant women. Patients who are asymptomatic after uncomplicated removal of a foreign body should be observed for a time in the emergency department and if they remain well may be discharged home. In the unconscious patient direct laryngoscopy should be performed before bag/valve/mask ventilation. This prevents the foreign body from being moved from a supraglottic to an intraglottic position. If no foreign body is visualized, the patient should be intubated and ventilated. If the patient cannot be ventilated due to airway resistance, the endotracheal tube should be advanced maximally. This aims to convert a complete tracheal obstruction to a main stem bronchus obstruction. The foreign body can then be removed in the operating theatre. Laryngotracheal trauma is rare, comprising 0.3% of all trauma presenting to emergency departments. The upper airway is relatively protected against trauma since the larynx is mobile and the trachea is compressible and because the head and mandible act as shields. Blunt trauma may be difficult to diagnose as external examination may be normal and there may be distracting head or chest injuries. ‘Clothes-line injuries’ involve cyclists or other riders hitting fences or cables. Direct trauma from assaults, sporting equipment or industrial accidents also occurs. Suicide attempts by hanging may cause traumatic injuries to the neck as well as airway obstruction due to the ligature. ‘Dashboard injuries’ occur when seatbelts are not worn, with sudden deceleration resulting in hyperextension of the neck and compression of the larynx between the dashboard and cervical spine. The most common laryngeal injury is a vertical fracture through the thyroid cartilage. Fractures of the hyoid bone and cricoid cartilage also occur and may be found in cases of manual or ligature strangulation. The cricothryoid ligament and the vocal cords may be ruptured and the arytenoids dislocated. Complete cricotracheal transection may occur. Up to 50% of patients sustaining significant blunt airway trauma have a concurrent cervical spine injury. Tracheal or laryngeal injury should be suspected if aphonia, hoarseness, stridor, dysphagia or dyspnoea occur. Patients may present with complete obstruction or may deteriorate rapidly after arrival. There may be minimal external evidence of injury or the larynx may be deformed or tender and there may be subcutaneous emphysema. It is important to check for associated head, chest and cervical spine injuries. Both laryngoscopy and bronchoscopy may be required. This should be performed in the operating theatre, as urgent surgical intervention may be indicated. X-rays should only be considered if the patient is stable with adequate ventilation. Lateral soft-tissue X-rays of the neck may provide information about airway patency, subcutaneous or soft-tissue emphysema and fractures of the hyoid and larynx. Elevation of the hyoid bone indicates cricotracheal separation. Plain X-rays may also confirm the presence of a foreign body. Cervical spine X-rays should be considered due to the association between upper airway injuries and cervical spine injuries. Chest X-rays may show signs of trauma and subcutaneous or mediastinal emphysema. CT of the neck is useful in assessing the extent of injuries to larynx, oesophagus, cervical spine and adjacent structures but should only be considered once the patient is stabilized. A classification system for severity of blunt upper airway injury based on endoscopic and radiological findings has been developed (Table 6.1.3). Table 6.1.3 Grading of blunt laryngeal injury Airway management with protection of the cervical spine is essential. Fibreoptic bronchoscopic intubation is preferable to minimize complications, such as laryngeal disruption, laryngotracheal separation or creating a false tracheal lumen. Cricothyrostomy is relatively contraindicated due to the altered anatomy. Emergency tracheostomy may even be required, ideally performed in the operating theatre. Early ENT involvement is important and indications for surgical exploration include airway obstruction requiring tracheostomy, uncontrolled subcutaneous emphysema, extensive mucosal lacerations with exposed cartilage as identified on bronchoscopic or laryngoscopic examination, vocal cord paralysis and grossly deformed, multiple or displaced fractures of the larynx, thyroid cartilage or cricoid cartilage. Mortality rates depend on the location of the injury, ranging from 11% for isolated fractures of the thyroid cartilage to 50% for injuries involving the cricoid cartilage, bronchi or intrathoracic trachea. Asphyxiation is the most common cause of death in blunt laryngeal trauma. Penetrating injuries may be secondary to assault or to sporting or industrial accidents. Other causes include eroding head and neck malignancies or post-radiotherapy. A focused history is mandatory. Penetration of the airway should be suspected if there is difficulty breathing, hoarseness or change in voice, stridor, pain on speaking, subcutaneous emphysema, haemoptysis or bubbling from the wound. Penetrating airway injury is often associated with great vessel or pulmonary injuries. Uncontrolled haemorrhage may lead to exsanguination as well as compromising the airway and requires prompt surgical intervention. As for blunt trauma (see above). Airway management with protection of the cervical spine is essential. Airway management is as for blunt trauma (see above). Early involvement of relevant surgical specialties is a priority. Burns may affect the airway by way of facial and perioral swelling, laryngeal oedema or constricting circumferential neck burns. Smoke inhalation occurs in about 25% of burn victims and may cause bronchospasm, retrosternal pain and impaired gas exchange. External examination may show evidence of burns. Carbonaceous material in the mouth, nares or pharynx suggests the possibility of upper airway thermal injury. If the patient presents with stridor or hoarseness, early intubation is essential because of the danger of increasing airway oedema and rapid progression to airway obstruction. Smoke inhalation may be associated with carbon monoxide poisoning and, in the setting of domestic or industrial fires, cyanide poisoning should also be considered. Endoscopy includes both laryngoscopy and bronchoscopy, performed in the operating theatre, as urgent surgical intervention may be required. Chest X-ray may show evidence of burn- associated acute respiratory distress syndrome (ARDS). Infections may involve the upper respiratory tract directly or adjacent structures. They range from the common and trivial to the rare and potentially life threatening. Croup and epiglottitis usually occur in children, but may be seen in adults. Acute respiratory infections are the most frequent reason for seeking medical attention in the USA and are associated with up to 75% of total antibiotic prescriptions there each year. Unnecessary antibiotic use can cause a number of adverse effects including allergic reactions, gastrointestinal upset, yeast infections, drug interactions, an increased risk of subsequent infection with drug resistant Streptococcus pneumoniae and added costs of over-treatment. Upper airway infections are generally diagnosed clinically. Symptom complexes where the predominant complaint is of sore throat are labelled pharyngitis or tonsillitis and, where the predominant symptom is cough, bronchitis. Acute respiratory symptoms in the absence of a predominant sign are typically diagnosed as ‘upper-respiratory-tract infections’. Each of these syndromes may be caused by a multitude of different viruses and only occasionally by bacteria. Most cases resolve spontaneously within 1–2 weeks. Bacterial rhinosinusitis complicates about 2% of cases and should be suspected when symptoms have lasted at least 7 days and include purulent nasal discharge and other localizing features. High-risk patients for developing bacterial rhinosinusitis or bacterial pneumonia include infants, the elderly and the chronically ill. Treatment should be symptomatic only. Antibiotic treatment does not enhance illness resolution nor alter the rates of complications. Sore throat is one of the top 10 presenting complaints to emergency departments in the USA. The differential diagnosis is large and includes a number of important conditions (Table 6.1.4). Table 6.1.4 Differential diagnosis of sore throat in the adult Infective pharyngitis Bacterial: Group A beta-haemolytic streptococcus most common pathogen. Diphtheria should be considered in patients with membranous pharyngitis Viral: including Epstein–Barr virus and herpes simplex virus Traumatic pharyngitis (exposure to irritant gases) Non-specific upper respiratory tract infection Quinsy (peritonsillar abscess) Epiglottitis Ludwig’s angina Parapharyngeal and retropharyngeal abscesses Gastro-oesophageal reflux Oropharyngeal or laryngeal tumour Pharyngitis has a wide range of causative viral and bacterial agents, most of which produce a self-limited infection with no significant sequelae. Group A beta-haemolytic streptococcus (Strep. pyogenes) (GABHS) is responsible for 5–15% of cases of pharyngitis in adults and, rarely, can trigger post-infectious syndromes of post-streptococcal glomerulonephritis and acute rheumatic fever. Clinical diagnosis of streptococcal pharyngitis is unreliable. Clinical prediction rules have been developed to help identify patients in whom evaluation with a throat culture or rapid antigen-detection test (RADT) is warranted. The most reliable clinical predictors for GABHS are the Centor criteria. One point each is allocated for the features of tonsillar exudate, tender anterior cervical lymphadenopathy or lymphadenitis, absence of cough and history of fever>38°C. One point is deducted for age>45 years. For a score of 0–1, no further testing or antibiotics is recommended. For scores of 2–3, further testing is recommended with antibiotics only given to patients with positive RADT or cultures. For a score of 4, empirical antibiotic treatment and/or further testing are advised. Rapid antigen tests have sensitivities ranging between 65 and 97%. Throat cultures take 2–3 days and may give false-positive results from asymptomatic carriers with concurrent non-GABHS pharyngitis. Serological testing is not useful in the acute treatment of pharyngitis but is useful in the diagnosis of rheumatic fever. The Infectious Diseases Society of America recommends throat cultures for children and adolescents with appropriate clinical criteria (fever, tonsillar exudates, tender cervical lymphadenopathy, absence of cough) but negative rapid antigen test. Adults with a negative RADT will not require cultures due to a lower incidence of GABHS pharyngitis and lower risk of rheumatic fever. Testing is not recommended for patients with clinical features suggestive of a viral aetiology (e.g. cough, oral ulcers, rhinorrhoea and hoarseness). Neisseria gonorrhoeae is an uncommon cause of pharyngitis and may be asymptomatic. It is seen in persons who practice receptive oral sex. N. gonorrhoeae pharyngitis is important to diagnose correctly both for appropriate treatment and because of the need to trace and treat contacts. HIV is an unusual cause of pharyngitis but should be considered in high-risk populations. The acute retroviral syndrome may present with an Epstein–Barr virus mononucleosis-like syndrome. Timely use of appropriate antibiotics prevents the development of acute rheumatic fever, decreases the duration of symptoms and decreases the incidence of suppurative complications, such as otitis media and peritonsillar abscesses. However, empirical antibiotic treatment on the basis of symptoms alone results in overuse of antibiotics, increased costs and an increased rate of side effects from antibiotics. Antibiotics have not been shown to decrease the incidence of post-streptococcal glomerulonephritis, which is related to the subtype of streptococcus. First-line antibiotics include oral penicillin V, amoxicillin, cephalexin, clindamycin or clarithromycin for 10 days or a single dose of intramuscular penicillin G. For uncomplicated pharyngeal gonorrhoea, ceftriaxone 125 mg IM as a single dose is the recommended treatment. Consideration should be given to concomitant treatment for Chlamydia if this has not been ruled out. Most patients with pharyngitis are managed as outpatients. Airway compromise is rare as the nasal passages provide an adequate airway. Some patients who are toxic or dehydrated may need admission for IV hydration and antibiotics. Penicillin or amoxicillin remain the drugs of choice for streptococcal pharyngitis. Regarding adjuvant corticosteroid therapy, a recent Cochrane review of patients with pharyngitis treated with antibiotics concluded that those with adjuvant corticosteroid therapy were three times more likely to experience complete resolution of their sore throat symptoms by 24 hours compared to those taking placebo. In addition, corticosteroids improved the time to onset of symptom relief and the time to complete resolution of symptoms. Adverse events, relapse rates and recurrence rates were not different for corticosteroid compared to placebo groups. Peritonsillar infections occur between the palatine tonsil, its capsule and the pharyngeal muscles. Peritonsillar cellulitis may progress to abscess formation. Cellulitis responds to antibiotics alone, but differentiating between the cellulitis and abscess and identifying those who require drainage may be difficult. Peritonsillar abscesses occur most commonly in males between 20 and 40 years of age. Symptoms include progressively worsening sore throat (usually unilateral), fever and dysphagia. On examination, the patient may have a muffled ‘hot potato’ voice, trismus, drooling, a swollen red tonsil with or without purulent exudate and contralateral deviation of the uvula. Clinical features do not always differentiate between quinsy and peritonsillar cellulitis. In such situations, imaging (e.g. CT), needle aspiration or trial of IV antibiotics help to differentiate between them. Complications include airway obstruction and lateral extension into the parapharyngeal space. Antibiotic therapy should include cover for GABHS, Staphylococcus aureus, Haemophilus influenzae and respiratory anaerobic species (Fusobacterium, Peptostreptococcus and Bacteroides). Appropriate antibiotics include penicillin V or clindamycin for patients allergic to penicillin. Needle aspiration in experienced hands can be useful but has a 12% false-negative rate and carries the risk of damaging the carotid artery. Formal surgical drainage or tonsillectomy may be necessary. Peripharyngeal ‘space’ infections have become rare in the post-antibiotic era but, of these, Ludwig’s angina or cellulitis of the submandibular space remains the most common. It was first described by Wilhelm Fredrick von Ludwig in 1836 and, at that time, was usually fatal because of rapid compromise to the airway. With prompt treatment, including IV antibiotics, the mortality rate has declined to less than 5%. Ludwig’s angina is classically bilateral. Infection may spread rapidly into adjacent spaces including the pharyngomaxillary and retropharyngeal areas and the mediastinum. Ludwig’s angina is related to dental caries involving the mandibular molars or it may be associated with peritonsillar abscess, trauma to the floor of the mouth or mandible and recent dental work. Cultures are usually polymicrobial and include viridans streptococci (40.9%), Staph. aureus (27.3%), Staph. epidermidis (22.7%) and anaerobes (40%), such as Bacteroides species. Clinical features include toothache, halitosis, neck pain, swelling, fever, dysphagia and trismus. Treatment necessitates admission and careful airway management. This may include endotracheal intubation as abrupt obstruction can occur. Surgical drainage is indicated if the infection is suppurative or fluctuant. The antibiotics of choice are high-dose penicillin plus metronidazole or clindamycin which should be administered IV. Parapharyngeal abscess involves the lateral or pharyngomaxillary space. Presentation and treatment are similar to Ludwig’s angina, from which they may develop. As well as the complications of Ludwig’s angina, including airway obstruction and spread to contiguous areas, there is the added risk of internal jugular vein thrombosis and erosion of the carotid artery which has a mortality of 20–40%. Retropharyngeal abscesses are more common in children below 5 years of age. In adults, they often result from foreign bodies or trauma. Presenting symptoms and signs include fever, odynophagia, neck swelling, drooling, torticollis, cervical lymphadenopathy, dyspnoea and stridor. Lateral neck X-rays show widening of the prevertebral soft tissues and sometimes a fluid level. CT of the neck may help in determining the extent and in differentiating an abscess from cellulitis. Magnetic resonance imaging (MRI), if available, is more sensitive than CT in assessing soft-tissue infections of the head and neck but demonstrates cortical bone poorly. Treatment requires admission, airway management, IV antibiotics and may include surgical drainage. Epiglottitis is becoming an adult disease although, in adults, there is significantly less risk to the airway than in children. The incidence of adult epiglottitis has remained relatively stable at 1–4 cases per 100 000 per year with a mortality of 7%. This may change over the next 10–20 years as vaccinated children grow into adolescents and adults. Acute adult epiglottitis is often referred to as supraglottitis because inflammation is not confined to the epiglottis, but also affects other structures, such as the pharynx, uvula, base of tongue, aryepiglottic folds and false vocal cords. H. influenzae has been isolated in 12–17% of cases and the high rate of negative blood cultures may reflect viral infections or prior treatment with antibiotics in cases that present late. Strep. pneumoniae, H. parainfluenzae and herpes simplex have also been isolated. Epiglottitis may also occur following mechanical injury, such as ingestion of caustic material, smoke inhalation and following illicit drug use (smoking heroin). Sore throat and odynophagia are the most common presenting symptoms. Other symptoms include fever and muffled voice. Drooling and stridor are infrequent. Factors shown to be associated with an increased risk of airway obstruction include stridor, dyspnoea, preferred upright posture and short duration of symptoms. A number of X-ray changes have been described in epiglottitis which are listed in Table 6.1.2. Antimicrobial therapy should provide cover against H. influenzae B, Strep. pneumoniae, beta-haemolytic streptococci and Staph. aureus. Third generation cephalosporins (ceftriaxone or cefotaxime) and antistaphylococcal agents active against methicillin-resistant Staph. aureus (MRSA) (e.g. clindamycin) should be used. The role of steroids and nebulized or parenteral adrenaline (epinephrine) in airway management is controversial. Most adults can be treated conservatively without the need for an artificial airway. Anne-Maree Kelly and Wee Yee Lee Asthma is a major health problem worldwide, resulting in significant morbidity and mortality. The prevalence of asthma varies significantly between regions across the world. In Australasia, New Zealand and the UK, it is thought to affect about 20% of children and 10% of adults. Sufferers tend to present to emergency departments when their usual treatment plan fails to control symptoms adequately. The respiratory compromise caused can range from mild to severe and life threatening. For these patients, the main role of the emergency care is therapeutic. Other reasons for patients with asthma to attend emergency departments (EDs) include having run out of medication, having symptoms after a period of being symptom and medication free and a desire for a ‘second opinion’ about the management of their asthma. For this smaller group, the primary role is one of educating about the disease, of planning an approach to the current level of asthma symptoms and of referral to appropriate health professionals, e.g. respiratory physicians or general practitioners. Asthma is a major health problem in many countries, resulting in significant morbidity and mortality. Data from the Global Initiative for Asthma suggest that more than 300 million people in the world are currently affected by asthma. The cost in terms of long-term medications and lost school and work days is difficult to quantify, but would run to millions of dollars annually. Australasia, the UK and North America have a greater prevalence of asthma than the Middle East and some Asian countries. There is also considerable geographical variation in severity, with Australasia reporting the highest proportion of severe disease. The reason for this geographical variation is unclear, but may relate in part to ethnicity, rural versus metropolitan environment and air pollution. A number of epidemiological studies suggest that the prevalence and severity of asthma is slowly increasing worldwide. Asthma is characterized by hyperreactive airways and inflammation leading to episodic, reversible bronchoconstriction in response to a variety of stimuli. It is a complex immunologically-mediated disease. There is strong evidence that it is inherited, although no single gene is directly implicated. A polygenic basis is likely to account for asthma’s wide clinical spectrum. Studies suggest that asthma sufferers may have abnormal immunological systems, innately hypersensistive airways and abnormal airway repair mechanisms. Environmental factors interact with this system to produce clinical disease. Triggers of the immunological response (e.g. an extrinsic allergen, viral respiratory tract infection, pollutants, occupational exposures, emotion, exercise and drugs, such as aspirin and β-blockers) result in an exaggerated inflammatory response with activation of cell types including mast cells, eosinophils, basophils, Th-2 cells and natural killer cells. This leads to the release of primary mediators, including histamine and eosinophilic and neutrophilic chemotactic factors and secondary mediators, including leukotrienes, prostaglandins, platelet-activating factor, interleukins and cytokines. These result in bronchoconstriction via direct and cholinergic reflex actions, increased vascular permeability (resulting in oedema) and increased mucous secretions. Studies suggest that airway remodelling occurs in asthma sufferers resulting in airways that are more hypersensitive than previously. It is postulated that this structural remodelling results in loss of lung function and loss of complete reversibility. Pathophysiologically the effects of acute asthma are: The aims of clinical assessment are confirmation of the diagnosis, assessment of severity and identification of complications. Asthma is characterized by episodic shortness of breath, often accompanied by wheeze, chest tightness and cough. Symptoms may be worse at night, which is thought to be due to variations in bronchomotor tone and bronchial reactivity. Attacks may progress slowly over days or rapidly over minutes. Atypical presentation includes cough and decreased exercise tolerance. Features suggesting an increased risk of life-threatening asthma include a previous life-threatening attack, previous intensive care admission with ventilation, requiring three or more classes of asthma medication, heavy use of β-agonists, repeated emergency department attendances in the last year and having required a course of oral corticosteroids within the previous 6 months. Behavioural and psychosocial factors have also been implicated in life-threatening asthma including non-compliance with medications, monitoring or follow up, self-discharge from hospital, frequent GP contact, psychiatric illness, denial, drug or alcohol abuse, obesity, learning difficulties, employment or income problems and domestic, marital or legal stressors. These should be sought in order to assess risk more accurately and plan management. Physical findings vary with the severity of the attack and may range from mild wheeze and dyspnoea to respiratory failure. Findings indicative of more severe disease include an inability to speak normally, use of the accessory muscles of respiration, a quiet or silent chest on auscultation, restlessness or altered level of consciousness, oxygen saturation on room air of<93% and cyanosis. Clinical features are a good guide to the severity of attacks. Features of the major severity categories are summarized in Table 6.2.1. Pulsus paradoxus has been abandoned as an indicator of severity. Table 6.2.1 Categorization of asthma severity based on clinical features Modified from Guidelines for Emergency Management of Adult Asthma, Canadian Association of Emergency Physicians, British Guideline on the Management of Asthma (SIGN) and Asthma Management Handbook (NAC) with permission. For mild and moderate asthma, investigations should be limited to pulmonary function tests (PEFR or FEV1). A chest X-ray is only indicated if examination of the chest suggests pneumothorax or pneumonia. Arterial blood gases are not useful in this group of patients. Assessment should include an assessment of PEFR if possible. For severe asthma, a chest X-ray is necessary as localizing signs in the chest may be hard to detect. Blood gas analysis may be useful if the oxygen saturation is less than 92% on room air at presentation, if improvement is not occurring as expected and if the patient appears to be tiring. For those with severe asthma, arterial blood gases may show:
Respiratory Emergencies
6.1 Upper respiratory tract
Introduction
Triage and initial evaluation
Upper-airway obstruction
Pathology
Clinical investigations
Endoscopy
Blood tests
Imaging
Neck X-rays
The ‘thumb’ sign
Oedema of the normally leaf-like epiglottis resulting in a round shadow resembling an adult thumb. The width of the epiglottis should be less than one-third the anteroposterior width of C4. In adults with epiglottitis, the width of the epiglottis is usually>9 mm
The vallecula sign
Progressive epiglottic oedema resulting in narrowing of the vallecula. This normally well-defined air pocket between the base of the tongue and the epiglottis may be partially or completely obliterated
Swelling of the aryepiglottic folds
Swelling of the arytenoids
Loss of the vallecular air space
Prevertebral soft tissue swelling
The width of the prevertebral soft tissue should be less than half the anteroposterior width of C4
Hypopharyngeal airway widening
The ratio of the width of the hypopharyngeal airway to the anteroposterior width of C4 should be less than 1.5
Computed tomography
Treatment
Foreign body airway obstruction
Treatment
Blunt trauma
Mechanisms of injury
Pathology
Clinical features
Clinical investigations
Endoscopy
Imaging
Plain X-ray
CT
Grade
Endoscopic and radiological findings
I
Minor laryngeal haematoma without detectable fracture
II
Oedema, haematoma or minor mucosal disruption without exposed cartilage, or non-displaced fractures on CT
III
Massive oedema, tears, exposed cartilage, immobile cords
Treatment
Prognosis
Penetrating trauma
Mechanism
Clinical features
Clinical investigation
Treatment
Thermal injury
Pathology and pathophysiology
Clinical features
Clinical investigations
Endoscopy
Imaging
Infections
Introduction
Non-specific upper airway infections
Pharyngitis/tonsillitis
Clinical investigations
Treatment
Quinsy/peritonsillar abscess
Epidemiology and pathology
Clinical features, investigations and complications
Treatment
Ludwig’s angina
Pathogenesis and pathology
Clinical features
Treatment and disposition
Other abscesses
Parapharyngeal abscesses
Retropharyngeal abscess
Epiglottitis
Epidemiology and pathology
Clinical features
Clinical investigations
Treatment
6.2 Asthma
Introduction
Epidemiology
Aetiology, pathophysiology and pathology
 increased physiological dead space
increased physiological dead space
 intrinsic positive end-expiratory pressure secondary to hyperventilation with air trapping.
intrinsic positive end-expiratory pressure secondary to hyperventilation with air trapping.
Clinical assessment
History
Examination
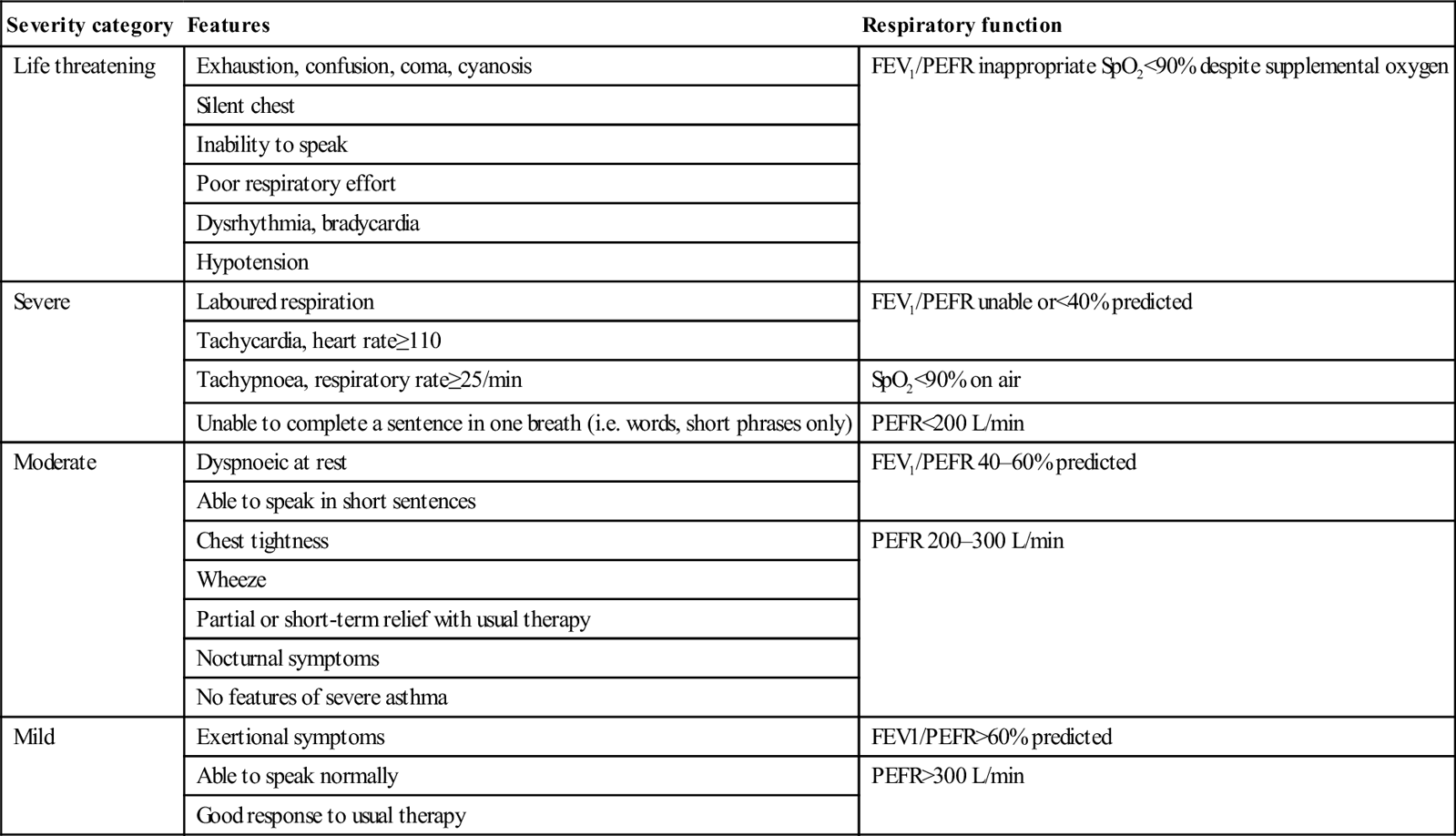
Severity category
Features
Respiratory function
Life threatening
Exhaustion, confusion, coma, cyanosis
FEV1/PEFR inappropriate SpO2<90% despite supplemental oxygen
Silent chest
Inability to speak
Poor respiratory effort
Dysrhythmia, bradycardia
Hypotension
Severe
Laboured respiration
FEV1/PEFR unable or<40% predicted
Tachycardia, heart rate≥110
Tachypnoea, respiratory rate≥25/min
SpO2<90% on air
Unable to complete a sentence in one breath (i.e. words, short phrases only)
PEFR<200 L/min
Moderate
Dyspnoeic at rest
FEV1/PEFR 40–60% predicted
Able to speak in short sentences
Chest tightness
PEFR 200–300 L/min
Wheeze
Partial or short-term relief with usual therapy
Nocturnal symptoms
No features of severe asthma
Mild
Exertional symptoms
FEV1/PEFR>60% predicted
Able to speak normally
PEFR>300 L/min
Good response to usual therapy
Clinical investigations
Mild to moderate asthma
Severe asthma
Chest X-ray
Blood gas analysis
< div class='tao-gold-member'>
Related posts:
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


6. Respiratory Emergencies









Only gold members can continue reading. Log In or Register to continue
