Edited by Anne-Maree Kelly and Anthony Brown Crispijn van den Brand and Anne-Maree Kelly Fractures of the clavicle account for 2.6–5% of all fractures and usually result from a direct blow on the point of the shoulder, but may also be due to a fall on the outstretched hand. The most common site of fracture is the middle third of the clavicle, which accounts for 69–82% of clavicular fractures. Most other clavicular fractures are in the outer third. There are varying degrees of displacement of the fracture ends, with overlapping fragments and shortening being common. Owing to the strategic location of the clavicle, injury to the pleura, axillary vessels and/or brachial plexus is possible but, fortunately, these complications are rare. They should be excluded by directed examination. The clinical signs of clavicular fracture are a patient supporting the weight of their arm at the elbow coupled with local pain and tenderness, often accompanied by deformity. In non-displaced or minimally displaced fractures, treatment consists of an elbow- supporting sling (e.g. broad arm sling) for 2–3 weeks. For comfort, this may be worn under clothes for the first few days. The sling may be discarded when local tenderness has subsided. Note that clinical union usually precedes radiological union by weeks. Early shoulder movement should be encouraged within the limits of pain and immobilization should be discontinued if clinical union has occurred, even if there is not yet radiological union. Non-union is rare. Midshaft fractures with complete displacement, comminution or fractures in the elderly or women with osteoporosis have a higher rate of non-union and poorer functional outcome. Recent evidence suggests that this group may benefit from surgical stabilization with either plate-and-screw fixation or intramedullary devices. Fractures of the outer third of the clavicle may involve the coracoclavicular ligaments. These fractures are generally displaced. If so, surgical management should be considered because these fractures have a high incidence of non-union (30%). Displaced fractures of the medial third of the clavicle are often associated with other serious injuries and warrant further examination. Early orthopaedic consultation is recommended for all (displaced) fractures of the medial and outer third of the clavicle. Late complications of clavicular fractures include shoulder stiffness and a local lump at the site of fracture healing, which is rarely of cosmetic significance. Acromioclavicular (AC) joint injuries usually result from a fall where the patient rolls onto his/her shoulder. The degree of the injury relates to the number of ligaments damaged; about two-thirds of AC injuries are incomplete and involve only part of the AC and coracoclavicular ligaments (CC) (types I and II). AC dislocations are classified according to the Tossy/Rockwood classification system (Fig. 4.1.1): On clinical examination of the standing patient, the outer end of the affected clavicle may be prominent and there will be local tenderness over the AC joint. The degree of damage can be ascertained by taking standing X-rays of both shoulders with the patient holding weights in both hands (stress X-rays) and by ultrasound. Stress X-rays may be normal in mild strains, but dynamic ultrasonographic techniques may better define the injury. Treatment is with a broad arm sling. For minor injuries (Rockwood type I/II) 1–2 weeks is usually sufficient. For type II injuries, heavy lifting and contact sports should be avoided for 4–6 weeks to avoid conversion to a type III injury. The treatment of type III injuries is controversial with some authors recommending conservative treatment and others surgery. Types IV to VI injuries are usually treated surgically. Sternoclavicular dislocations are uncommon and usually due to a direct, high velocity blow to the medial clavicle or medial compression of the shoulder girdle. Subluxation is more common than dislocation, with the affected medial end of the clavicle displaced forwards and downwards. Dislocations may be anterior or, rarely, posterior. In the latter case, the great vessels or trachea may be damaged. Clinical features include local tenderness and asymmetry of the medial ends of the clavicles. The diagnosis is essentially clinical. X-rays are difficult to interpret and are not necessary for subluxations. For dislocations, contrast enhanced CT scanning should be obtained. Subluxations should be treated in a broad arm sling for 2–3 weeks. Anterior sternoclavicular joint instability should also be treated conservatively; however, there is a significant risk of ongoing instability that is usually well tolerated and of little, if any, functional impact. For patients with posterior dislocation, expeditious diagnosis and treatment are important. Closed reduction, performed under general anaesthesia, is usually stable and the joint can then be managed in a brace or sling for 4–6 weeks. Operative stabilization is required if closed reduction is unsuccessful or there is persistent instability. Fractures of the scapula are uncommon, accounting for less than 1% of all fractures. They typically occur after high-energy trauma. Up to 90% of patients have other associated injuries. Fractures of the blade of the scapula are most common and are usually due to direct violence. Clinical features are local tenderness, sometimes with marked swelling. Healing is usually rapid, even in the presence of comminution and displacement, with an excellent functional outcome. Treatment is usually non-operative, with a broad arm sling and early mobilization. There is growing acceptance of surgical treatment for highly displaced fractures. However, there is no evidence comparing outcome for surgical versus non-surgical treatment. Fractures of the scapula neck are often comminuted and may involve the glenoid. Swelling and bruising of the shoulder may be marked. Clinical examination and X-rays should ensure that the humeral head is enlocated. Computed tomography (CT) scans may be useful in defining the anatomy and the degree of involvement of the glenoid, including any steps in the articular surface. Surgery is often indicated for fractures involving the scapular neck or glenoid. The ‘floating shoulder’ is an uncommon injury pattern. Although it is usually defined as an ipsilateral fracture of the clavicle and scapular neck, recent studies suggest that ligamentous disruption associated with a scapular neck fracture can give the functional equivalent of this injury pattern, with or without an associated clavicle fracture. Because the degree of ligament disruption is difficult to assess, indications for non-surgical and surgical management are not well defined. Minimally displaced fractures typically do well with conservative management. The degree of fracture displacement and ligament disruption that results in poor outcome with conservative management is not well defined and the indications for surgery are controversial, as is choice of surgical technique. Options include fixation of the clavicular fracture, which often indirectly reduces the scapular fracture, or fixation of both fractures. Rotator cuff tears most commonly affect the supraspinatus tendon and become more common with advancing age as degeneration weakens the cuff. Indeed, the presence of asymptomatic partial or complete tears identified on ultrasound or magnetic resonance imaging (MRI) may be as high as 40% in patients aged over 50. Symptomatic injuries may follow minor trauma or the sudden application of traction to the arm. Many are acute or chronic in nature, rather than truly acute. This can be defined with ultrasound or MRI if required. The clinical features of a strain include a painful arc of abduction centred at 90° of abduction, weakness in external rotation and tenderness under the acromion. If the tear is complete, no abduction at the glenohumeral joint will occur, although some abduction to 45–60% is possible by scapular rotation. In both partial and complete injuries, there is a full passive range of abduction. Another useful test to isolate the supraspinatus and test its integrity is the ‘empty can’ test. The patient abducts the arm to 30° with 30° of forward flexion and full internal rotation (i.e. thumb pointed down) and is then asked to forward flex the shoulder first without and then against resistance. Pain or weakness against resistance suggests supraspinatus injury. The goals of emergency care for rotator cuff injuries are to provide pain relief and prevent further disability. For the acute symptoms, an arm sling can provide support but prolonged immobilization should be avoided. Treatment of supraspinatus tears is controversial, with no clear evidence guiding the choice of operative versus non-operative therapy or the components or duration of non-operative treatments. Most experts would still recommend a trial of non-operative therapy before considering surgery. An exception to this may be the patient with a previously asymptomatic shoulder who sustains trauma with resultant weakness (after the pain from the injury subsides) in whom imaging studies indicate an acute full-thickness tear. Dislocation of the shoulder results in the humeral head lying anterior, posterior or inferior to the glenoid. Of these, anterior dislocation is the most common. Anterior glenohumeral dislocation is most often due to a fall resulting in external rotation of the shoulder, for example, the body rotating internally over a fixed arm. It is most common in young adults, often being related to sports. There is inevitable damage to the joint capsule (stretching or tearing) and there may be associated damage to the subscapularis. Anterior dislocations are associated with several fractures including Hill–Sachs deformities, (bony) Bankart lesions and greater tuberosity fractures. A Hill–Sachs deformity is an impression fracture of the humeral head caused by the glenoid and is present in 35–100% of all anterior dislocations. It is unclear if this is prognostically important. Bony Bankart lesions are caused by a disruption of the glenoid labrum with an avulsion of the glenoid. These occur in about 5% of patients. Another common fracture is of the greater tuberosity of the humerus. Other complications may include damage to the axillary (circumflex) nerve (resulting in inability to contract deltoid and numbness over the insertion of deltoid) and, rarely, the axillary vessels and the brachial plexus. Clinical features include severe pain, reluctance to move the shoulder and the affected arm being supported at the elbow, often in slight abduction. The contour of the shoulder is ‘flattened off’ and there is a palpable gap just under the acromion where the humeral head usually lies. The displaced humeral head may be palpable anteriorly in the hollow behind the pectoral muscles. Dislocation is confirmed by X-ray. The dislocation may be evident on the AP film but cannot be ruled out on a single view. Additional views (e.g. an axial lateral, translateral, tangential lateral) are required. These may reveal an associated fracture of the greater trochanter, but this does not influence initial management. The principles of management are the provision of adequate analgesia as soon as possible, reduction of the dislocation and immobilization followed by physiotherapy. There are more than 20 described methods for the reduction of anterior dislocations, with reported success rates ranging from 60 to 100%. These include the FARES technique, the Spaso technique, the modified Kocher’s manoeuvre, the Milch technique and scapular rotation techniques (www.youtube.com/watch?v=NXFPWxSTK5c). There is no high-quality evidence to assist in selecting the most effective method. That said, the Hippocratic method is not recommended as the traction involved may damage neurovascular structures. Gravitational traction (the Stimson technique), having the patient lie face down with a weight strapped to the limb, is occasionally successful and may be worthwhile if there will be a delay until reduction by another method. All reduction methods require adequate analgesia. Intra-articular local anaesthetic may also be useful. Sedation, in an appropriately controlled environment, may be of assistance in augmenting analgesia and providing a degree of muscle relaxation and amnesia, but is not required in most cases. Failure of reduction under analgesia/sedation is rare and mandates reduction under general anaesthesia. If there is an associated fracture of the greater trochanter, it usually reduces when the shoulder is reduced. If it remains displaced, open reduction and internal fixation may be required. Post-reduction X-rays confirm reduction and neurovascular status must be rechecked. Post-reduction care includes immobilization in a broad arm sling followed by physiotherapy. Available evidence suggests that there is no benefit from immobilization for more than 1 week. It was suggested that bracing in external rotation might reduce the incidence of recurrent dislocation but this has not been borne out in validation studies. Primary surgery, usually by arthroscopic techniques, is recommended for patients having suffered recurrent dislocations and should be considered for first-time dislocators, especially those who are young, as surgery has been shown to significantly reduce the risk of recurrent dislocation. Recurrence is rare in the elderly, but is common (64–68%) in young patients. Most anterior glenohumeral dislocations can be reduced without anaesthesia or procedural sedation, although appropriate analgesia and a patient, gentle technique is required. Intra-articular lignocaine (lidocaine) has been shown to be a safe, effective alternative to procedural sedation for reduction of dislocated shoulders. The patient may be in the supine or prone position. Hold the patient’s wrist and apply traction to the affected limb in a neutral position. Move the limb anteriorly and posteriorly in small oscillating movements (about 5–10 cm) while continuing to apply traction slowly abducting the limb. Once the limb is abducted to 90°, externally rotate the limb at the shoulder, with ongoing traction and oscillating anterior/posterior movements. Continue slowly to abduct the limb past this position. Reduction is usually achieved once the limb is abducted to about 120°. Success rate of the order of 89% has been reported. The patient is placed in the supine position. The affected arm is held by the forearm or wrist and gently lifted vertically, applying traction. While maintaining vertical traction, the shoulder is then externally rotated, resulting in reduction. If necessary, countertraction by downward pressure over the shoulder joint may be applied. Success rate of the order of 75% has been reported. While applying traction to the arm by holding it at the elbow, the shoulder is slowly externally rotated, pausing if there is muscle spasm or resistance. External rotation to about 90° should be possible and reduction often occurs during this process. The elbow is then adducted until it starts to cross the chest and then internally rotated until the hand lies near the opposite shoulder. This technique is traditionally performed with the patient prone, but can be performed on a seated patient. For both variations, the scapula is manipulated by adducting (medially displacing) the inferior tip using thumb pressure while stabilizing the superior aspect with the other hand. Posterior dislocation is frequently mentioned in medicolegal reports as it is easy to miss, especially in the unconscious patient. It may result from a fall on the outstretched or internally rotated hand or from a blow from the front. It is also associated with seizures and electrocution injuries, where it is not uncommonly bilateral. The dislocation is usually not apparent on an AP film, so additional views are required. Reduction is performed by traction on the limb in the position of 90° abduction, followed by external rotation. Aftercare is the same as for anterior dislocation. Posterior dislocation is prone to recurrence. Good functional outcomes are associated with early detection and treatment, a small osseous defect and stability following closed reduction. Poor prognostic factors include late diagnosis, a large anterior defect in the humeral head, deformity or arthrosis of the humeral head, an associated fracture of the proximal part of the humerus and the need for an arthroplasty. The indications for surgery are controversial. This type of dislocation is rare and usually obvious, as the arm is held in abduction. Neurovascular compromise is a significant risk requiring careful examination and prompt reduction. Reduction is by traction in abduction followed by swinging the arm into adduction. Aftercare is the same as for anterior dislocation. Controversies Raymond Chi Hung Cheng and Timothy H Rainer The function of the upper limb depends on an intact shoulder girdle that is, in turn, affected by the integrity of muscles, tendons and ligaments, bones, joints, blood vessels and nerves. Fractures of the humerus severely limit efficient function of the upper limb and may be divided into proximal (proximal to the surgical neck), middle (shaft) and distal (supracondylar) segments. Fractures of the proximal humerus represent 5% of all fractures presenting to emergency departments (ED) and 25% of all humeral fractures. The fracture typically occurs as a result of an indirect mechanism in elderly, osteoporotic patients who fall on their outstretched hand with an extended elbow. The majority do not require surgical intervention and may initially be treated in the ED. A subset with a non-viable humeral head requires early surgical intervention and it is therefore important to identify this group. Fractures of the humerus may also occur in patients with multiple injuries or in the elderly with associated fractures of the neck of femur. Patients typically present soon after injury holding their arm close to the chest wall. They complain of pain and exhibit swelling and tenderness of the shoulder and upper arm. Although crepitus and bruising may occur, the former should not be elicited because it causes excessive and unnecessary pain. Bruising is usually delayed, occurring several days after injury. It appears around the lower arm rather than at the fracture site as a result of gravity and blood tracking distally. A neurovascular examination is essential as the axillary nerve, brachial plexus and/or axillary artery may be damaged. The axillary nerve is the most commonly injured and presents with altered sensation over the badge area (insertion of the deltoid) and reduced deltoid muscle contraction (which may be hard to assess because of pain). The axillary artery is the commonest vessel to be injured and may present with any combination of limb pain, pallor, paraesthesia, pulselessness and paralysis. As these injuries frequently occur in elderly patients, careful attention must be paid to the reason for the fall, as an underlying acute medical condition may have precipitated the event and require management in its own right. Three radiographic views – anteroposterior, lateral and axillary – will allow most proximal humeral fractures to be correctly diagnosed. Although the majority of these fractures are easily managed in the ED, the challenge is to differentiate these from the minority that require orthopaedic intervention. In this system, fractures are classified first according to the number of the four anatomical sites (humeral head, humeral shaft, greater and lesser tuberosities) that were involved in the injury; second, according to the degree of fracture displacement, defined as 1 cm separation or>45° angulation (Figs 4.2.1 and 4.2.2). One-part fracture One-part fractures account for 80% of proximal humeral fractures. Any number of fracture lines may exist, but none are significantly displaced. Two-part fracture Two-part fractures account for 10% of proximal humeral fractures and one fragment is significantly displaced or angulated. Two-part fractures of the humerus may involve the anatomical neck (see Fig. 4.2.1A), the surgical neck (see Fig. 4.2.1B), the greater tuberosity (see Fig. 4.2.1C) or the lesser tuberosity (see Fig. 4.2.1D). Three- and four-part fractures Three-and four-part fractures account for the remaining 10% of proximal humeral fractures, with two or three significantly displaced or angulated fragments (see Fig. 4.2.2A–C). One-part fractures and two-part fractures can be treated with a collar and cuff sling, adequate analgesia and follow up. Early mobilization is important and the prognosis is good. Definitive management of the displaced fragment in two-part fractures may include open or closed reduction depending upon neurovascular injury, rotator cuff integrity, associated dislocations, likelihood of union and function. Early orthopaedic assessment is recommended. For three- and four-part fractures, the consensus is for open reduction and internal fixation. However, a review has suggested that there is little evidence that surgery is superior to the non-operative approach. For displaced proximal humeral fractures, surgical management remains varied and controversial. A recent systematic review suggested that non-operative treatment of proximal humerus fractures has a high rate of radiological healing, good functional outcomes but a lower complication rate when compared with the operative approach. Small, randomized controlled trials suggest that external fixation may confer some benefit over closed manipulation and that conservative treatment is better than tension band osteosynthesis. Another study suggests that the decision should be made according to the viability of the humeral head. Locking plate technology may also provide better outcomes in patients with unstable displaced humeral fractures having a viable humeral head. Other small-scale studies suggest that some bandaging styles may be better than others and that early physiotherapy may improve functional outcome. Fractures at these sites are uncommon, but are important to recognize as they have a high incidence of compromised blood supply to the articular segment, may result in avascular necrosis and may require a humeral hemiarthroplasty. Fractures of the greater tuberosity accompany 15% of anterior glenohumeral dislocations and may be associated with rotator cuff tears. Although the fracture may be grossly displaced, reduction of the dislocated shoulder usually also reduces the fracture. In patients who require the full range of movement of their shoulders, surgical repair of the cuff may be required. Fractures of the lesser tuberosity are associated with posterior glenohumeral dislocations. Most patients with undisplaced one- and two-part fractures may be discharged from the ED with a collar and cuff sling, analgesia, early mobilization and appropriate follow up. High-risk cases, including displaced three- and four-part fractures, all open fractures and the special proximal humeral fractures described above, require orthopaedic consultation and admission, as do those with medical problems requiring investigation or treatment. Low-energy fractures, especially in the elderly, suggest the presence of osteoporosis. ‘At-risk’ patients not already identified as having osteoporosis should be referred for bone density scans, vitamin D testing and treatment. Fractures of the humeral shaft commonly occur in the third decade (active young men) and in the seventh decade of life (osteoporotic elderly women). The commonest site is the middle third, which accounts for 60% of humeral fractures. The close proximity of the fracture to the radial nerve and brachial artery commonly leads to neurovascular deficits. Direct blows tend to produce transverse fractures, whereas falls on the outstretched hand produce torsion forces and hence spiral fractures. Combinations of the two mechanisms may produce a butterfly segment. Pathological fractures are also common, most resulting from metastatic breast cancer. The angle and degree of displacement of the fracture depends on the site of injury and its relationship to the action and attachment of muscles on either side of the injury (Fig. 4.2.3). Patients typically present complaining of pain and supporting the forearm of the injured limb, flexed at the elbow, and held close to the chest wall. Examination of the limb reveals tenderness, swelling, shortening and possibly deformity. The skin should be assessed for tension or disruption and particular attention should be paid to the shoulder and elbow regions for associated fractures or dislocations. Initial and post-reduction assessments of the brachial artery and vein and ulnar, median and radial nerves are essential. The commonest complication is radial nerve injury resulting either from the injury itself or reduction of the fracture and is evidenced by wrist drop and altered sensation in the first dorsal web space. A recent systemic review reported that radial nerve injury occurs in 11% of midshaft humerus fractures. Two radiographic views – anteroposterior and lateral – will allow the correct diagnosis in most cases. Uncomplicated, closed fractures account for the majority of injuries and may be treated conservatively by immobilization and analgesia. Immobilization can be by a hanging cast, U-shaped cast or with functional bracing and a broad arm or collar and cuff sling. The acceptable deformity is 20° anterior/posterior angulation and 30° valus/valgus deformity. The rate of fracture union is usually higher than 90%. Early specialist follow up is recommended. Some authors prefer a functional humeral brace rather than U-shaped plaster for immobilization, as the former may permit greater functional use without affecting healing or fracture alignment. For oblique/spiral fractures, some orthopaedic surgeons prefer an operative approach for a better functional outcome. Open fractures and complications affecting the vessels require surgical repair. Although the majority of radial nerve injuries are neuropraxia and recover without surgical intervention, each case should be considered individually by an orthopaedic surgeon with a view to possible operative exploration. Unlike in children, fractures of the distal humerus in adults are very uncommon and patterns of injury tend to reflect the anatomical two-column construction (condyles) of the humerus. Several classification methods have been used, such as the Riseborough and Radin, Mehne and Matta classifications, but the simplest and most commonly used are the AO/ASIF classifications. These classify injuries into three categories: type A are extra-articular fractures, type B are partial articular and type C are complete articular fractures. Practically, distal humeral fractures may be classified into supracondylar, intercondylar and other types. Supracondylar fractures lie transversely, whereas intercondylar T or Y fractures include an additional vertical extension between the condyles. Mechanisms of injury usually involve a direct blow to the flexed or extended elbow. In the former, the olecranon is driven upwards, thereby either splitting the condyles apart producing a ‘T’ or a ‘Y’ pattern, or shearing off one condyle. Patients typically present with a swollen, tender, deformed elbow. As very little subcutaneous or other tissue separates the bone from skin, any disruption of the skin should be carefully examined for the possibility of a compound fracture. Distal neurological and vascular injury must be assessed carefully, as the possibility of nerve injury has been reported to be as high as 12–20%. Two radiographic views – anteroposterior and lateral – should be obtained. Some authors suggest that an internal oblique view may improve the diagnostic accuracy. Pain and inability to extend the elbow often result in poor-quality radiographs. Although high-quality radiographs are essential for operative planning, repeat films should not be attempted in the ED as they rarely provide the desired result. When there is any suspicion of severe injury, either from the history or from gross soft- tissue swelling, early computed tomography (CT) scanning should be considered to give better detail, especially of intra-articular fractures. Undisplaced fractures may not be visible on radiography but may be suggested by posterior or anterior fat pad signs, which result from fat displaced by an underlying haemarthrosis. Ultrasonography, CT and magnetic resonance imaging may all improve diagnostic precision. They alter management and improve outcome in patients with occult fractures, mostly of the intra-articular type. Uncomplicated, undisplaced, closed fractures with minimal swelling should be immobilized for 3 weeks in 90° flexion with an above-elbow cast and a broad arm sling, followed by active mobilization. Patients with severe swelling, compound fractures, displaced fractures or neurovascular compromise require orthopaedic intervention. Raymond Chi Hung Cheng and Timothy H Rainer Elbow dislocation, along with glenohumeral and patellofemoral joint dislocations, is one of the three most common large joint dislocations. The elbow joint is a hinge-like articulation involving the distal humerus and proximal radius and ulna. Owing to its strong muscular and ligamentous supports, the joint is normally quite stable and rarely requires operative intervention, even for acute instability after dislocation. Elbow dislocations can be classified as either anterior or posterior. Posterior dislocation is the most common type and can be further divided into posteromedial or posterolateral. It usually results from a fall on the outstretched hand with some degree of flexion or hyperextension at the elbow. The radius and ulna commonly dislocate together. Similarly, anterior dislocation can also be divided into anteromedial or anterolateral. This type is less common and is usually due to a direct blow to the dorsal side of the elbow. Uncommonly, the radius or ulna alone may dislocate at the elbow. In such cases, there is always a fracture of the other bone. One common example is in Monteggia fractures, where anterior or posterior radio-humeral dislocation occurs alongside a fracture of the proximal one third of the ulna shaft (Fig. 4.3.1). A rarer example is a posterior ulna-humeral dislocation with fracture of the radial shaft. So, although elbow dislocations may appear to be isolated, it is essential to look for associated intra-articular or shaft fractures. Patients typically present holding the lower arm at 45° to the upper arm and there is swelling, tenderness and deformity of the elbow joint. The three-point anatomical triangle of olecranon, medial and lateral epicondyles should be assessed for abnormal alignment, as this strongly suggests dislocation. The commonest neurovascular injury involves the ulnar nerve, reported in 10–15% of elbow dislocations, but the median and radial nerves and the brachial artery may also be affected. The differential diagnosis is a complex distal humerus fracture which, in a swollen elbow, may be hard to differentiate clinically from an elbow dislocation. Anteroposterior and lateral radiographic views should be obtained and scrutinized for associated fractures of the coronoid process, radial head, capitellum and olecranon. Magnetic resonance imaging (MRI) characterizes bony injury more accurately than radiography in children with elbow injuries, but its potential role for diagnosis and guiding management in adults has not been well evaluated. Duplex Doppler ultrasound can be use to identify early brachial artery injury. Simple dislocation can be reduced using a closed method. With adequate sedation, gentle traction and counter-traction, the joint relocates quite easily. Medial and posterolateral dislocations may also require sideways correction. Dislocation of the stable elbow joint produces severe soft-tissue injury and resultant instability, therefore, after reduction, signs and symptoms of compartment syndrome should be sought. Joint instability should be tested by valgus and varus testing and by lateral pivot-shift test. The reduced elbow joint should move smoothly. Any crepitation or resistance, particularly during the mid-range, suggests incongruent reduction or soft tissue interposition, which is commonly associated with coronoid process or epicondylar fractures. Inability to fully flex or extend the elbow suggests a loose bone or cartilaginous fragment or a capsular tear. Post-reduction films should be assessed, not only for correct joint relocation, but also for associated fractures. After successful reduction, the elbow should be placed in a posterior plaster slab in 90° of flexion. Cylinder casts are contraindicated because of the likelihood of severe soft-tissue swelling. There is little evidence that surgical intervention improves outcome in patients with medial or lateral elbow instability after dislocation. A recent systematic review found that there is no difference in outcome between surgical repair of the ligament and plaster immobilization for simple elbow dislocation. Patients with functional treatment have a better range of movement, less pain, better functional scores, shorter disability and shorter treatment time when compared with plaster immobilization. The management of Monteggia fracture- dislocation is discussed in Chapter 4.4. Compound fracture dislocation should be reduced by the open method. Patients with irreducible dislocations, neurovascular complications, associated fractures or open dislocations require orthopaedic intervention. Ulnar nerve injuries can occur both before and after closed reduction. The reported rate varies between 10 and 15%. Most of them are neuropraxia and will recover with conservative measures. The most sensitive sign and symptoms are numbness over the little fingers. Current practice is that most patients may be discharged from the emergency department with analgesia, pressure bandage for stable joints and plaster immobilization for unstable joints. A broad arm sling with appropriate follow up should be arranged after reduction. A recent prospective, randomized study suggested that early mobilization is superior to plaster immobilization in terms of functional recovery, without any increased instability or a recurrence of dislocation for patients with uncomplicated posterior dislocations. The duration of immobilization should not be longer then 14 days to prevent joint stiffness. Patients with irreducible dislocations, neurovascular complications, associated fractures or open dislocations require admission. Crispijn van den Brand Radial head fractures occur frequently, usually as a result of a fall onto an outstretched hand or, less frequently, following a direct blow to the lateral side of the elbow. Radial head fractures present with pain and restricted movement at the elbow. Usually, there is swelling and tenderness over the radial head. Sometimes, with more subtle injuries, rotating the forearm while palpating the radial head may be necessary to elicit tenderness. Elbow extension and forearm rotation are limited. Severely comminuted fractures may have proximal displacement of the radius, which can be associated with disruption of the interosseous membrane and subluxation of the distal radioulnar joint (Essex–Lopresti fracture dislocation). Standard anteroposterior (AP) and lateral X-rays of the elbow are required. A radiocapitellar view may be necessary if the fracture is subtle. The presence of an anterior fat pad sign alone on X-ray is associated with an underlying radial head or neck fracture in up to 50% of patients. In this case, a fracture should be assumed to be present if there is an appropriate mechanism and local signs. A follow-up X-ray or computed tomography (CT) scan is indicated only in the presence or persistent pain, stiffness or locking. Radial head fractures are usually classified according to the (modified) Mason classification (Fig. 4.4.1). About two-thirds of fractures are Mason type I. The Mason classification is as follows: All non-displaced (type I) radial head fractures and those type II fractures without mechanical block may be managed with a bandage and sling. Mobilization should be started as early as possible. If there is severe pain, a posterior splint may be useful but should not be applied for more than 2 days. Prognosis is good, but full extension may not be possible for many months. Displaced or complex radial head fractures (type II or III) may be treated in the acute setting with a sling or posterior splint. These patients should have early orthopaedic review (within days). The treatment of displaced or complex radial head fractures remains controversial and should be determined by an orthopaedic surgeon. Mechanical block can be difficult to assess acutely due to pain. Intra-articular injection of bupivacaine may assist early assessment or assessment may be deferred until pain has settled. Surgical options include open reduction and internal fixation and excision of the radial head with or without implantation of a prosthesis. Radial neck fractures with up to 20° tilts can be managed conservatively. More severe tilt can be reduced using intra-articular local aneasthesia. The forearm is pronated until the most prominent part of the radial head is felt. Then traction is applied to the forearm and pressure applied to the radial head. Open reduction is indicated if closed methods fail or displacement is severe. Neurovascular complications and compartment syndrome are uncommon. Most complications relate to disturbance of the relationships of the proximal radio-ulnar and radiocapitellar articular surfaces causing limitation of movement. This is uncommon with minor fractures. This type of injury requires great force, typically from a motor-vehicle accident, a fall from a height or a direct blow. These fractures are commonly open and nearly always displaced. The forearm is swollen and tender and may be angulated and rotated. Examination looking for an open wound, local neurovascular compromise, compartment syndrome or musculotendinous injury is required. Given the mechanism of injury, other injuries should also be sought. AP and lateral X-rays of the forearm, including the wrist and elbow joints, are needed. Displacement and angulation are easily determined, but torsional deformity may be subtle. Because the ulna and radius are rectangular in cross-section rather than circular, a change in bone width at the fracture site indicates rotation. The radial and ulnar styloid processes normally point in opposite directions to the bicipital tuberosity and coronoid process, respectively. A change in this alignment also suggests torsion. Adult forearm fractures are less stable than those in children and lack of remodelling limits tolerance to incomplete reduction. Undisplaced fractures may be managed with an above- elbow cast, but must be reviewed at 1 week for displacement and angulation. Most fractures, however, are displaced and require open reduction and internal fixation. Early complications include wound infection, osteomyelitis, neurovascular injury and compartment syndrome. Later, non-union, malunion, reduced forearm rotation and reflex sympathetic dystrophy are possible complications. These fractures are due to a direct blow to the ulna, often when raised in defence; hence they are also known as ‘nightstick’ fractures. Patients present with localized pain and swelling. AP and lateral X-rays delineate the location of the fracture and degree of angulation. Look for associated dislocation of the radial head if displacement is present (Monteggia fracture dislocation). Fractures displaced less than 50% of the ulna width heal well with a non-union rate of 0–4%. Traditional treatment involves fixing the forearm in mid-pronation with a plaster cast, extended above elbow if the middle or proximal thirds of the ulna are fractured. The cast is removed once union occurs, usually in about 8 weeks. Other proven options include a below-elbow plaster (BEPOP) for proximal fractures, early mobilization with bandage after 1–2 weeks in BEPOP or functional bracing after 3–5 days, which allows movement at wrist and elbow. Fractures with more than 10° of angulation or displaced more than 50% of the diameter of the ulna require surgical intervention. This is a rare fracture of the proximal ulna with dislocation of the radial head. It occurs either through a fall onto the outstretched hand with hyperpronation or through a force applied to the posterior aspect of the proximal ulna. Patients present with pain, swelling and reduced elbow movement. The forearm may appear shortened and the radial head may be palpable in the antecubital fossa. Associated posterior interosseous nerve injury is common. On X-ray the fracture is obvious, but the dislocation is commonly missed. Check that a line through the radial shaft bisects the capitellum on both views. There are four types of Monteggia fracture depending upon displacement of the radial head (Bado classification). Dislocation is anterior in 60% (Bado type I), but may be lateral or posterior. All Monteggia fractures require open reduction and internal fixation. Common complications include malunion and non-union of the ulnar fracture and an unstable radial head. Isolated fractures of the proximal two-thirds of the radial shaft are uncommon and are usually displaced. Rare undisplaced fractures can be treated similarly to isolated ulnar shaft fractures. Displaced fractures require open reduction and internal fixation. Fractures of the distal third of the radial shaft occur as a result of a fall onto the outstretched hand or a direct blow. There may be an associated subluxation or dislocation of the distal radioulnar joint (DRUJ), known as the Galeazzi fracture dislocation. Patients have pain and swelling at the radial fracture site. Those with a Galeazzi injury will also have pain and swelling at the DRUJ and a prominent ulnar head. X-rays show the radial fracture, which is tilted ventrolaterally. Widening of the DRUJ space on the AP X-ray and dorsal displacement of the ulnar head on the lateral X-ray are seen (Fig. 4.4.2). An ulnar styloid fracture is seen in 60% of cases.
Orthopaedic Emergencies
4.1 Injuries of the shoulder
Fractures of the clavicle
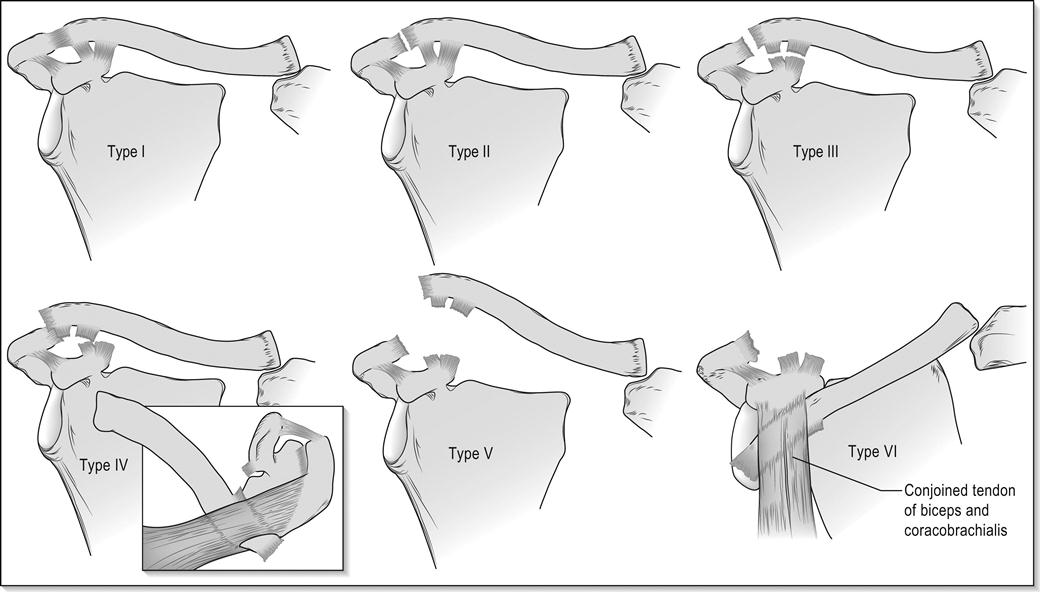
Acromioclavicular joint injuries
Sternoclavicular subluxation and dislocation
Fractures of the scapula
Supraspinatus tendon injuries
Dislocation of the shoulder
Anterior dislocation
Reduction techniques (www.youtube.com/watch?v=NXFPWxSTK5c)
FARES technique
Spaso technique
Modified Kocher’s manoeuvre
Scapular rotation
Posterior dislocation
Inferior dislocation (luxatio erecta)
 The role of surgery for midshaft clavicular fractures.
The role of surgery for midshaft clavicular fractures.
 Optimal treatment for Rockwell type III AC joint disruptions.
Optimal treatment for Rockwell type III AC joint disruptions.
 Surgical treatment of scapular fractures.
Surgical treatment of scapular fractures.
 Immobilization method after reduction of dislocation of the shoulder.
Immobilization method after reduction of dislocation of the shoulder.
 The best technique for reduction of anterior dislocation of the shoulder.
The best technique for reduction of anterior dislocation of the shoulder.
4.2 Fractures of the humerus
Introduction
Fractures of the proximal humerus
Patterns of injury
Clinical assessment
Clinical Investigations
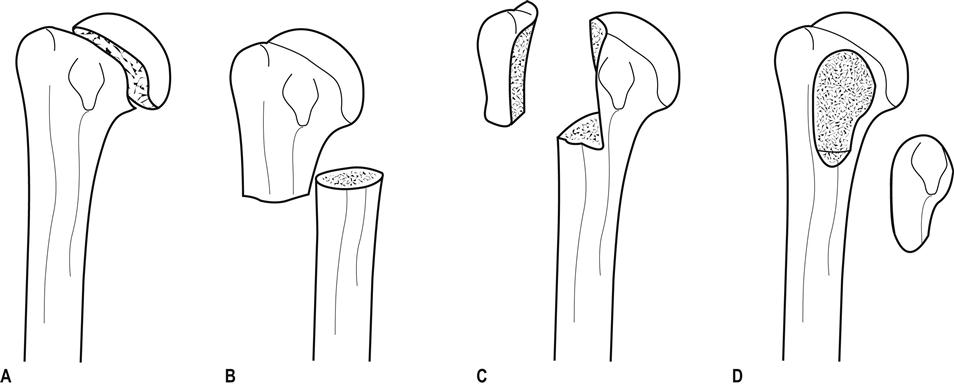
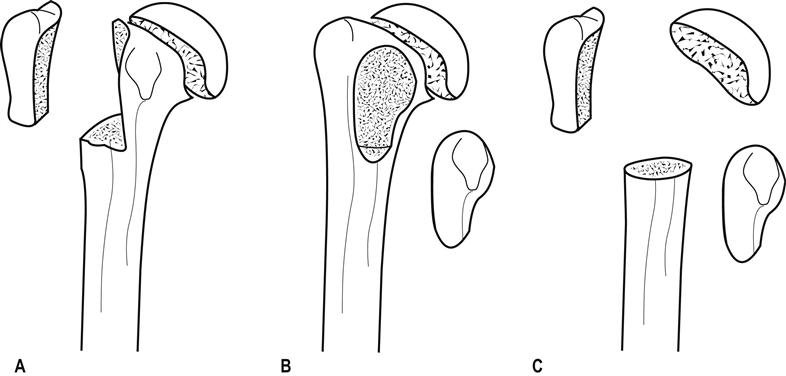
Fracture classification
Neer classification system
Treatment
Special cases
Fracture of the anatomical neck and articular surface
Fracture dislocations
Disposition
Fractures of the shaft of humerus
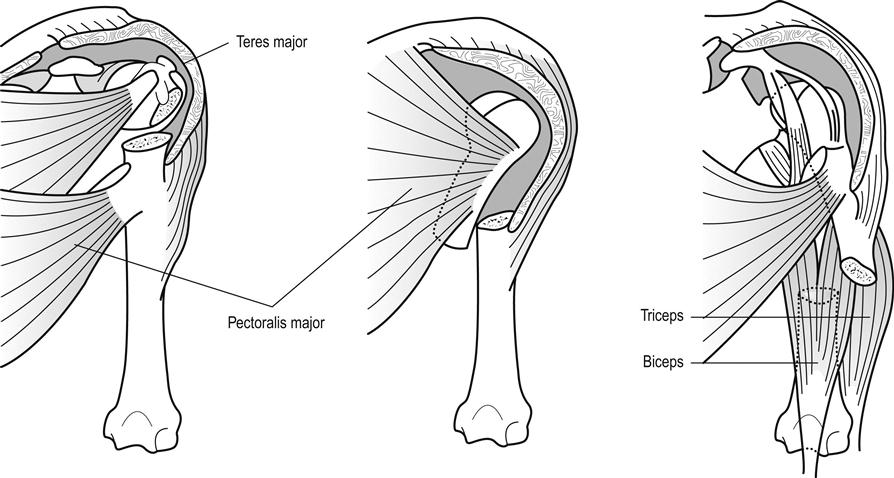
Patterns of injury
Clinical assessment
Clinical investigations
Treatment and disposition
Fractures of the distal humerus
Classification and patterns of injury
Clinical assessment
Clinical investigations
Treatment and disposition
4.3 Dislocations of the elbow
Introduction
Clinical assessment
History and examination
Clinical investigations
Treatment
Disposition
4.4 Fractures of the forearm and carpal bones
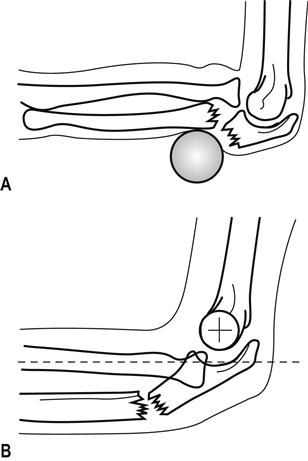
Radial head fractures
Clinical features
History
Examination
Clinical investigations
Imaging
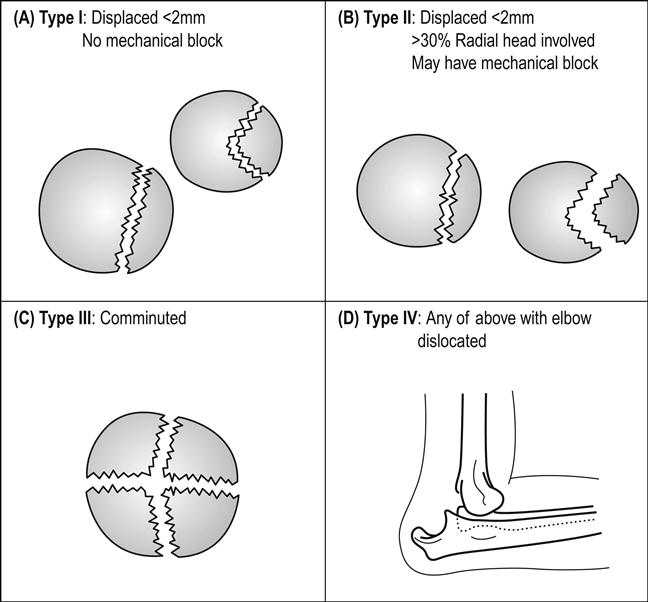
Classification
Treatment
Complications
Shaft fractures
Clinical features
History
Examination
Clinical investigations
Imaging
Treatment
Complications
Specific fracture types
Isolated fracture of the ulnar shaft
Monteggia fracture dislocation
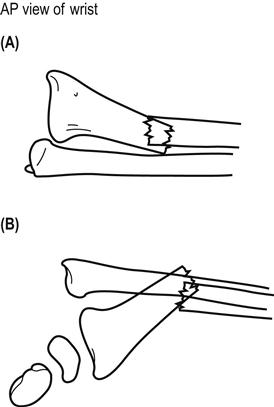
Isolated radial shaft fracture
Galeazzi fracture dislocation
Related posts:
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree