Edited by Peter Cameron Peter Cameron and Gerard O’Reilly Trauma is the leading cause of death from 1 to 44 years of age in developed countries. The burden of injury is especially high in developing countries, where systems of trauma care are generally non-existent [1,2]. Globally, road traffic crashes are the number one killer of young people [3]. Deaths from unintentional injury are much more common than suicide or homicide, even in the USA [1]. However, in the USA, homicide causes more deaths than suicide in the 15–24-year age group [1]; this differs from other developed countries. Suicide now causes more deaths than motor vehicle accidents (MVAs) in regions such as Australasia and the UK [4,5]. Morbidity due to injury affects a much larger group. The 2010 Global Burden of Disease Study showed that injuries cost the global population some 300 million years of health every year, causing 11% of disability-adjusted life years (DALYs) worldwide [3]. The economic and social costs are great as most victims are young and are major contributors to society through their work, family and organizational involvement. In most developed countries, there have been significant reductions in mortality and morbidity due to injury as a result of a systematic approach to trauma care [6,7]. The majority of these reductions have resulted from prevention strategies, including seatbelt legislation, drink–driving legislation, improved road engineering, motor cycle and cycle helmet use and road safety and workplace injury awareness campaigns. Changes in both trauma system configuration and individual patient management have brought about improvements in the survival rate of those who are seriously injured, although the impact has not been as great as that of injury prevention. Civilian interest in injury morbidity and mortality was initially most evident in the USA because of the high incidence of urban violence and road trauma and because of lessons learnt from the wars of the 20th century. Research into systems of trauma care began with epidemiological work by Trunkey and others examining trauma deaths [8]. These researchers developed the concept of a trimodal distribution of trauma deaths. Trunkey proposed that about 50% of deaths occurred within the first hour as a result of major blood vessel disruption or massive CNS/spinal cord injury. This could only be improved by prevention strategies. A second more important group (from the therapy perspective) accounted for about 30% of deaths and included patients with major truncal injury causing respiratory and circulatory compromise. The remaining 20% of patients were said to die much later from adult respiratory distress syndrome, multiple organ failure, sepsis and diffuse brain injury. Trunkey initially identified the second group as most likely to benefit from improvements in trauma system organization and it is a tribute to the effectiveness of such schemes that the number of patients dying from avoidable factors within the first few hours of injury has generally declined. In some systems, it is reported to be as low as 3% but, generally, is probably nearer to 10–15% [9,10]. Improvements in trauma system provision have resulted in a redistribution of the three groups proposed by Trunkey and it is now generally accepted that far fewer than 30% are included in the second group. In fact, more recent studies have shown that complications, such as multiple organ failure (MOF) and acute respiratory distress syndrome (ARDS), have decreased to such an extent, with improved initial management, that, in mature trauma systems, even the third peak is now minimal, with the vast majority of deaths occurring in the first 1–2 hours from major head injury and massive organ disruption [11]. Trauma care systems have been developed to ensure a multidisciplinary approach and a continuum of care from the roadside through hospital care to rehabilitation. Identifying weakness in such a system is always difficult because of the delay between cause and effect. Inappropriate management does not usually lead to immediate death: for example, a period of hypoxia may result in organ failure many hours later. Another difficulty is the relatively low incidence of death. Although this is of course to be welcomed, it does make statistical analysis more difficult when the ‘adverse event’ occurs uncommonly. Careful audit of the entire trauma process and accurate measurement of ‘input’ (i.e. injury severity) and ‘output’ (i.e. death or quality of survival) is essential if the process of trauma care is to be reviewed. Whereas the initial work on trauma system development focused on the need for centres of expertise and trauma management, it is now accepted that the pre-hospital phase is of critical importance. The linchpin of a mature trauma system is a highly skilled and resourced pre-hospital service following the key principle of ‘the right patient to the right hospital in the shortest time’ [12]. Timely triage of the injured patient to the closest most appropriate facility is essential. Specifically, high-risk patients should be taken to a hospital capable of managing critically ill trauma patients [12]. A diagrammatic representation of one integrated trauma system, at its inception in 1999, is provided in Figure 3.1.1[13]. Criteria for identifying those patients who may require resuscitation at a tertiary level Trauma Centre or ‘Major Trauma Service (MTS)’ will depend on resources. In the most developed trauma systems, ‘mechanism of injury’ criteria are usually included in the pre-hospital triage tool. This ensures high sensitivity of the tool, but leads to considerable overtriage. In less-resourced settings, it may be appropriate to identify high-risk patients on the basis of abnormal vital signs and obvious major injury. The elements of a trauma system’s triage tool may include most or all of the predictors of life-threatening injury listed in Table 3.1.1. Table 3.1.1 Predictors of life-threatening injury appropriate for use in pre-hospital trauma triage The appropriate application of pre-hospital triage guidelines relies upon adequate resourcing. In regions with developed trauma systems, pre-hospital staff are expected to provide a range of advanced life support interventions including patient intubation and chest decompression, thereby ensuring that further organ injury is limited during the pre-hospital phase. The pre-hospital care providers armed with these skills may be doctors (as in many European countries) or highly trained paramedics (as in the USA, Australia and the UK). Effective pre-hospital communication, usually by phone and/or radio, allows timely preparation for the arrival of a trauma patient. Proper communication includes trauma team notification, staff and trauma bay identification and the adoption of universal precautions (gloves, gowns, etc.). Trauma team notification might occur by phone or paging system and ensures the gathering of the trauma team prior to the patient’s arrival. Members of the trauma team may vary. An example of trauma team composition and roles in a Level 1 Trauma Centre is provided in Box 3.1.1. Variations to this list may occur in different settings depending upon the availability of skilled staff and the nature of specific injuries or physiological status prior to the patient’s arrival Trauma team call-out criteria reflect the pre-hospital trauma triage criteria (see Table 3.1.1) and should be applied rigorously. Trauma team skill, functioning and leadership are essential to achieve the best patient outcome. The appropriate skill mix is reflected by the team membership listed in Box 3.1.1. Trauma team performance, including leadership and communication, will have an impact on patient outcome. The application of a consistent systematic approach to trauma resuscitation has been widely promulgated by training programmes, such as the Advanced Trauma Life Support (ATLS) [14]. The patient is brought directly to a prepared bay, the layout of which is illustrated in Figure 3.1.2. The principles of the initial identification and management of immediately life-threatening injuries, with prioritization accorded to airway (including protection of cervical spine), breathing, circulation, (neurological) disability and exposure are applied to all injured patients. This is followed by a secondary survey involving a head-to-toe examination. In most departments, parallel processing of the patient will occur simultaneously with management of ABCDE problems. It should be assumed that hypoxia is present in all patients who have sustained multiple injuries. Early expert airway intervention is essential. Every patient should receive initial supplemental oxygen via a well-fitting face-mask. If the airway is clear and protected, the neck should be immobilized with a semi-rigid collar but, if airway manoeuvres are necessary, it is often better to use manual inline immobilization without a collar, ensuring minimal neck movement with constant vigilance. The management of an obstructed airway in a trauma patient should be undertaken by an experienced senior clinician with significant anaesthetic experience. The first priority is to clear the upper airway by direct visualization, suction and removal of any foreign bodies. Insertion of an oropharyngeal or nasopharyngeal airway and the jaw-thrust manoeuvre are usually successful in clearing an upper airway obstruction. Insertion of a nasopharyngeal airway can be hazardous in patients with a fracture of the cribriform plate. The direction of insertion (backwards not upwards) is important. Chin lift is not recommended because it may cause additional movement of the cervical spine. Early endotracheal intubation should be undertaken if the patient is apnoeic, has an unrelieved upper airway obstruction, has persistent internal bleeding from facial injuries, has respiratory insufficiency due to chest or head injuries or the potential for airway compromise (airway burns, facial instability, coma or seizures). Intubation may also be necessary for procedures such as computed tomography (CT) scanning or for the management of confused or disturbed patients. Any operator undertaking emergency intubation of major trauma victims should be skilled in rapid sequence induction and prepared for a difficult intubation. He/she must also be equipped with the skills for dealing with a ‘failed’ intubation (see Chapter 2.1) with a variety of interventions, including surgical cricothyroidotomy. Once the airway is secure, the patient’s breathing needs to be assessed. Particular attention is paid to optimizing oxygenation and maintaining normocapnia. During the primary survey, immediately life-threatening risks to breathing must be identified and dealt with. These injuries include tension pneumothorax, open pneumothorax, massive haemothorax, flail and pulmonary contusion. The specific features and management of these injuries is covered in Chapter 3.6. Shock is a clinical syndrome in which the perfusion of vital organs is inadequate to maintain function. Blood loss is the major cause of shock in the major trauma patient. Other less common causes of shock also need to be considered: The initial stages of hypovolaemia can be difficult to detect. Reliance on systolic blood pressure to identify shock is dangerous. All patients who have sustained an injury that could be associated with significant blood loss, however remote the possibility, must be carefully monitored. In the initial phase, measurement of the clinical parameters will give some information about vital organ perfusion. However, more invasive monitoring will be required if hypovolaemia is severe or sustained. It is essential to gain good venous access at the earliest phase in resuscitation. This is usually via two large-bore peripheral cannulae. In the absence of accessible arm veins, central venous access may be indicated. The recommended site (subclavian, jugular or femoral) depends on a number of factors. The subclavian vein is reliable in terms of patency, while the ease of access to the femoral vein is offset by its potential futility in major truncal haemorrhage. The internal jugular veins can be difficult to access in the immobilized trauma patient. Cut-downs of the saphenous veins and cubital fossa may also be used. At the initial stages, where the blood pressure is unchanged, patients with potential blood loss can usually be managed without blood transfusion, namely crystalloid. There has been no benefit demonstrated in using non-blood colloids over crystalloids in traumatic haemorrhage [15–17]. Similarly, for hypertonic crystalloid the available data are inconclusive [18]. Where there is hypotension and tachycardia, blood transfusion should commence immediately, initially using O-negative blood and changing to group-specific or cross-matched blood as it becomes available. Chapter 3.12 covers the role and details of massive transfusion therapy in the trauma patient. Conversely, until the source of haemorrhage has been identified and haemostasis achieved, vigorous over resuscitation with fluid may actually result in a worse outcome [19,20]. The essential point is that after securing the airway and optimizing oxygenation and ventilation, the most important determinant of outcome in the major trauma patient with haemorrhagic shock is the time to definitive haemostasis. There is certainly no point in delaying surgery ‘to normalize the intravascular volume’. The major source of haemorrhage in the trauma patient must be identified early. The usual suspects are chest, abdomen, pelvis, long bone and/or external (e.g. scalp, major limb artery). As the purpose of the primary survey is to identify immediate threats to life, the assessment for a head injury and its severity entails an examination of conscious state (Glasgow Coma Score) and neurological signs (pupils, limb weakness). If there is any risk of intracranial injury, a CT brain scan will be indicated immediately upon completion of the primary survey. Chapter 3.2 deals with the assessment and management of traumatic brain injury. Hypothermia is associated with worse outcomes in the major trauma patient [21]. Temperature control is now considered to be of critical importance in reducing the sequelae of major trauma (metabolic derangement, coagulopathy). The role of therapeutic hypothermia in isolated head injury remains controversial and is a subject of ongoing research. While maintaining normothermia, it is important to have fully exposed the patient, including a log roll with spinal immobilization, to enable a complete examination. By this stage, the trauma patient will have been received into a well-organized resuscitation area and the first life-saving procedures will have been initiated by an integrated and skilled team of doctors and nurses. Any immediately life-threatening conditions can be expected to have been identified and dealt with. Constant vigilance and reassessment are essential. Other occult injuries may be present in those patients identified with serious injuries. While the trauma team leader continues to review the situation in the light of a constantly changing clinical scenario and, hopefully, the provision of more biomechanical data from the site of the incident, he or she should also be beginning to consider the next steps. The first of these is the calling in of other experts. Whereas it will have been clear that an airway doctor will be an essential part of the initial resuscitation team, it may be some minutes before it is known which other skills are required. Usually orthopaedic surgeons and neurosurgeons are near the top of the list. General surgery is not required as often as is commonly supposed [22], although general surgeons are often useful in coordinating ongoing care. Whichever specialty is required, the patient’s emergency problems demand experience, therefore, ‘if in doubt, refer’. Radiographs are required at this stage. The initial films should be limited to those that will have a direct bearing on immediate management, including a chest AP view and a pelvis AP view. Lateral X-ray of the cervical spine is no longer mandatory at this stage of assessment. Cervical immobilization is routine and it is not possible to exclude cervical injury with a lateral cervical spine X-ray. Therefore, a cervical X-ray does not alter initial management. Its utility at this stage would be to confirm an irretrievable injury, i.e. craniocervical dislocation. Ideally, the resuscitation room should have an integrated X-ray facility but, if this is not available, portable films should be obtained. It is not appropriate to transfer a multiply injured unstable patient to a separate X-ray facility. Other forms of imaging have become popular in localizing the source of haemorrhagic shock. The increasing availability of the focused assessment with sonography in trauma (FAST) has superseded diagnostic peritoneal lavage (DPL) as the bedside adjunct for detecting intraperitoneal haemorrhage. Following the primary survey and investigations deemed necessary, the patient requires a secondary survey, the full head-to-toe examination for injuries not classified as immediately life-threatening. Subsequent chapters deal with individual trauma problems, but it is essential that throughout the patient’s stay in hospital a single clinician has overriding responsibility for his or her care. In the resuscitation area, this is the ‘team leader’, who may be from any trauma-related discipline. Handover to the clinician responsible for ongoing care must be comprehensive, timed and well documented. Trauma kills people in a variety of ways; hence no one department in a hospital will see a large number of deaths. Many trauma victims die before they reach hospital, some in the ED and others scattered through the inpatient specialties and in intensive care. Hence from any one clinician’s perspective, trauma is not an outstanding problem. However, when looked at from a public health perspective, it is clearly a major issue, not least because some of the deaths are avoidable. Identifying these and the much more difficult-to-define group of patients who survive but whose outcome is not as good as expected is a major problem. The most important variables to measure are the extent of the anatomical injury, the degree of physiological derangement that results, age and the previous well-being of the patient. All these have a direct effect on outcome and must therefore be measured before any comment can be made about the process of care. Outcome itself must also of course be measured. This is relatively easy in terms of mortality. However, disability is a much more difficult issue and, currently, there are no universally accepted measurement tools. The Glasgow Outcome Scale (GOSE) [23, 24], and the Short Form–36 (SF36) questions [25] are available tools that have been used. As 90% of major trauma patients survive their injury in a mature trauma system, it is important to measure disability and quality of life following major trauma when comparing outcomes [26]. Trauma audit was first formalized by Champion at the Washington Hospital Centre in the 1970s, using the Trauma Injury Severity Score (TRISS) methodology [27,28]. Most current trauma systems are now audited using some approach to examining risk-adjusted mortality. Injury severity adjustment, allowing intra- and intersystem comparison, usually requires measures of anatomical injury (e.g. Injury Severity Score), physiological effects (e.g. Revised Trauma Score) and age. Globally, national governments are beginning to recognize the burgeoning human and economic cost of trauma, particularly road trauma. The public health achievements of the developed countries (seatbelts, helmets, alcohol and speed restrictions) are being implemented and, similarly, governments of developing countries are looking to implement trauma systems [29,30]. Research in developing countries reinforces the benefits of trauma systems previously described in countries with established emergency medical systems. For example, evidence indicates that people with life-threatening but potentially treatable injuries are up to six times more likely to die in a country with no organized trauma system than in one with an organized, resourced trauma system [31]. Trauma system development requires trauma outcome measurement [32,33]. As such, developing countries are likely to adopt trauma registries over the next several decades in an attempt to track the burden of trauma and the impact of system-wide interventions. As developing countries embark upon trauma system development, it is becoming increasingly important to access standardized trauma care education through intensive short-courses. Advanced Trauma Life Support (ATLS) has been widely used. Other courses (such as Primary Trauma Care (PTC)) have also become popular in the developing world. Such courses are often less expensive and more flexible than ATLS. Gerard O‘Reilly, Lee Wallis and Peter Cameron Neurotrauma is a common feature in the presentation of multisystem trauma, particularly when associated with motor vehicle accidents and falls. Over 50% of trauma deaths are associated with head injury. The implications for the health system are enormous, with an annual rate of admission to hospital wards associated with head trauma approaching 300 per 100 000 population [1] and twice this in the elderly [2]. The long-term sequelae of moderate and severe neurotrauma are a major health resource drain and the morbidities associated with mild brain injury are becoming clearer. Advances in preventative strategies, trauma systems, resuscitative therapies and rehabilitation management have improved outcomes. However, neurotrauma remains a serious health issue, predominantly affecting the productive youth of society. Primary brain injury occurs as a result of the forces and disruptive mechanics of the original incident: this can only be avoided through preventative measures, such as the use of bicycle helmets. Secondary brain injury is due to a complex interaction of factors and typically occurs within 2–24 hours of injury [3]. A principal mechanism of secondary injury is cerebral hypoxia due to impaired oxygenation or impaired cerebral blood flow. Cerebral blood flow is dependent on cerebral perfusion pressure (CPP), mean arterial systemic blood pressure (MAP) and intracranial pressure (ICP). Intracranial pressure may be raised as a result of the mass effect of the haemorrhage or by generalized cerebral oedema. Cerebral vasospasm further reduces cerebral blood flow in patients in whom significant subarachnoid haemorrhage has occurred. Cellular dysfunction is a result of both primary and secondary mechanisms and involves sodium, calcium, magnesium and potassium shifts across the cell membrane, the development of oxygen free radicals, lipid peroxidation and glutamate hyperactivity. Excessive release of excitatory neurotransmitters and magnesium depletion also occur [4]. Primary injuries are classified as: The significance of skull fracture is not related to the specific bony injury but rather the associated neurotrauma. Fractures in the region of the middle meningeal artery in particular may be associated with acute extradural haemorrhage. Fractures involving the skull base and cribriform plate may be associated with CSF leak and the risk of secondary infection. Depressed skull fractures may compress underlying structures, cause secondary brain injury and require surgical elevation. Injury to underlying structures may result in secondary epilepsy. Concussion is a transient alteration in cerebral function, usually associated with loss of consciousness and often followed by a rapid recovery. The proposed mechanism is a disturbance in the function of the reticular activating system. Post-concussive syndromes, including headache and mild cognitive disturbance, are common [5,6]. Symptoms, particularly headache, are usually short-lived but may persist. ‘Second-impact syndrome’ describes a greater risk of significant re-injury following an initial injury causing a simple concussion. It is likely to be due to diffuse cerebral swelling [7]. In animal models, concussion may be associated with modest short-term increases in intracranial pressure and disturbances in cerebral cellular function [8]. Cerebral contusion is bruising of the brain substance associated with head trauma. The most common mechanism is blunt trauma. Forces involved are less than those required to cause major shearing injuries and often occur in the absence of skull fracture. Morbidity is related to the size and site of the contusion and coexistent injury. Larger contusions may be associated with haematoma formation, secondary oedema or seizure activity. The most common sites for contusions are the frontal and temporal lobes [9]. Extradural haematoma (EDH) is uncommon but classically associated with fracture of the temporal bone and injury to the underlying middle meningeal artery. Haemorrhage subsequently occurs, stripping the dura from the skull and expanding to cause a rise in intracranial pressure and eventually uncal herniation and death. Haemorrhage may be from vessels other than the middle meningeal artery (e.g. brisk arteriolar or venous bleeding). Signs will depend on the site of the haematoma. Subdural haematomata (SDH) may have an acute, subacute or chronic course. It generally follows moderate head trauma with loss of consciousness. In the elderly, SDH may be associated with trivial injury and, in children, with shaking (abuse) injury. Haemorrhage occurs into the subdural space, slowly enlarging to cause a space-occupying collection whose functional implications will vary according to location. Acute subdural haemorrhage carries a high mortality (>50%), similar to acute EDH. Subacute and chronic SDH is associated with a degree of cerebral dysfunction, headache or other symptomatology and is associated with a significantly lower mortality (up to 20%) [10]. As with cerebral contusion, the most common sites of intracerebral haemorrhage associated with trauma are the temporal and posterior frontal lobes. Effects on function are variable, depending on the site. Intracerebral haemorrhage may progress from an initial contusion or be secondary to altered vascular characteristics. Symptom development and complications may be delayed as the size of the haemorrhage increases over time. Subarachnoid blood is relatively common after major head injury. Intraventricular haemorrhage may also be evident. As in non-traumatic settings, the presence of subarachnoid blood may lead to cerebral vasospasm and secondary ischaemic brain injury. Diffuse axonal injury (DAI) is the predominant mechanism of injury in neurotrauma, occurring in up to 50% of patients [11]. Shearing and rotational forces on the axonal network may result in major structural and functional disturbance at a microscopic level. Disturbance to important communicative pathways sometimes results in significant long-term morbidity, despite non-specific or minimal changes on computed tomography (CT) scanning. The exact pathogenesis of diffuse axonal injury is incompletely understood. Specific injury in the regions of the corpus callosum and midbrain has been proposed; however, DAI is believed to be the mechanism for persistent neurological deficits seen in head-traumatized individuals with normal CT scans [12]. Penetrating neurotrauma is characterized by high levels of morbidity and mortality. This is especially true of gunshot wounds. Exposure of cerebral tissue through large compound wounds or through basilar skull structures is associated with a dismal outlook. Penetrating injury in the periorbital and perinasal regions is associated with high risk of infection. Neurotrauma is surprisingly common. In some settings, more than 30% of the population have suffered from a trauma brain injury. In addition to being a major cause of death in trauma, neurotrauma leads to significant morbidity. More than 40% of those who have sustained a traumatic brain injury will have residual disability one year later [13]. Common causes include motor vehicle accidents (including vehicle versus pedestrian and bicycle collisions), falls, assault and firearms. In young males, alcohol is often involved. Primary prevention of neurotrauma depends on the cause. Most preventative strategies are directed at vehicular traffic and include speed-calming measures, in-car safety devices and bicycle helmets. Improving roadside lighting and enhancing pedestrian visibility contribute to reduction of injury in this group. Prevention of secondary injury involves maintenance of cerebral perfusion and oxygenation and is addressed under clinical management. Neurotrauma may be classified according to severity as minimal, mild, moderate or severe (Box 3.2.1) [14]. Such a classification allows for directed investigation and management, but there is clearly a continuum of injury within the spectrum of neurotrauma. A detailed history of the mechanics of the trauma is essential. This should be followed by consideration of time courses, pre-hospital care, pre-sedative and pre-relaxant neuromuscular function and episodes and duration of hypotension or other decompensation. A history of previous health problems, allergies, medications and social setting is desirable. As with all trauma patients, the initial assessment and therapy must be directed at maintenance of airway, ventilation and circulatory adequacy along standard Advanced Trauma Life Support (ATLS) principles. Early assessment of neurological disturbance using the Glasgow coma score (GCS) or AVPU scale (Alert: GCS 14–15; response to Verbal stimuli: GCS 9–13; response to Painful stimuli: GCS 6–8; or Unresponsive: GCS 3–5) is important. Simultaneous protection of the cervical spine by immobilization is fundamental. This management should commence in the pre-hospital setting and the level of care be maintained. The greatest risks to the patient with a moderate to severe head injury are hypoxic injury and deficient cerebral perfusion due to systemic hypotension. A full secondary survey, including log-roll, should follow. Clinical assessment of the neurological status of head-injured patients commences with formal documentation of the GCS (Table 3.2.1). The maximum score is 15 and the minimum 3. Coma may be defined in terms of the GCS, in which patients have a total score of 8 or less: Table 3.2.1 Examination of pupillary responses, particularly in the unconscious patient, is important as an indicator of increasing intracranial pressure; a non-responsive dilated pupil indicating ipsilateral herniation. However, a more common cause of abnormal pupil reactions in head injury is the presence of direct ocular trauma. A general neurological examination, including reflexes, should be performed; the degree to which cooperation is possible and lateralization of signs being particularly important to document. Consideration of the pre-injury mental state is important, particularly where drug or alcohol intoxication is possible. In head injury associated with loss of consciousness or amnesia and a GCS of 14–15, CT scanning will demonstrate a relevant positive scan (i.e. cerebral contusion, haematoma, oedema, pneumocephalus) in 7–12% and a subsequent craniotomy rate of 1–3% [15–18]. On the weight of research evidence, current ED investigation of mild head injury should include CT scanning in all patients in this group [14,19–22]. Certain high-risk groups (such as the intoxicated, the elderly (>65 years), anticoagulated or demented patients) warrant CT scanning even after minimal presumed or possible head injury. Despite considerable research within the minimal–mild head injury group, reliable risk stratification has not been achieved. The Canadian Head Rules detail five high-risk criteria for neurosurgical intervention in patients with GCS 13–15 and mild head injury [23]. The NICE head injury rules were based in part on the Canadian rules [24]; the NEXUS II [25] investigators showed that development of a simple head injury CT rule that is both sensitive and specific is extremely difficult. There have been conflicting results as to which has the best predictive power in adults and children, however, each has its critics for over-scanning [26,27]. Cervical spine imaging is indicated if the patient has neck pain, neurological abnormality, altered conscious state, intoxication or significant distracting injury. Urgent CT scanning is the investigation of choice in moderate-to-severe neurotrauma (GCS of 3–13); however, other investigations and therapy may take priority in the patient with multisystem trauma, particularly in the presence of unresponsive haemorrhagic shock. In the absence of a CT scan, consultation with a neurosurgeon or early transfer to an appropriate facility is essential. Imaging of the cervical spine is indicated in all patients with moderate to severe neurotrauma. A significant proportion of patients with severe head injury will have cervical spine fractures. All patients with mild head injury must be counselled appropriately and discharged with written advice in the care of a responsible adult. Specific advice must be provided regarding expected duration of symptoms, possible risks or delayed complications and reasons for re-presentation to the ED (Box 3.2.2). Information should also be given about the second-impact syndrome and exclusions from sporting activity. Box 3.2.2 General advice following head injury The patient should read and understand these instructions: Report immediately the following problems Follow up by a local medical officer should be arranged and neuropsychological assessment may be warranted for high-risk groups. Patients should be cautioned about making major life, occupational and financial decisions until they are free of post-concussive symptoms. In minimal and mild head injury, a normal CT scan and the absence of neurological abnormality are reasonable criteria for patient discharge [3]. It is essential to assess for ongoing post-traumatic amnesia (PTA), as this is frequently overlooked in the ED. A simple screen to use is the modified Westmead PTA scale [6]. In the presence of these criteria, the persistence of mild symptoms (e.g. mild headache, nausea, occasional vomiting) is common and patients should be advised accordingly. In adults, such symptoms may be treated with mild analgesics (paracetamol, aspirin) and antiemetics (metoclopramide, prochlorperazine) and the patient discharged when comfortable. Advising patients that there will be problems with post-concussive symptoms (including short-term memory and information processing) and providing them with written material has been shown to improve outcomes at 3 months [6,28]. Currently there is no drug to treat the primary pathology in mild and minor head injury [29]. Priority in the management of moderate to severe neurotrauma is given to maintenance of the airway and an adequate cerebral perfusion pressure. Hypotension (SBP<90) and hypoxia (PaO2<60 [8 kPa]) should be corrected immediately [30]. Control or modification of intracranial pressure has a place in the emergency management of neurotrauma. Avoidance of secondary brain injury and associated cerebral swelling is the mainstay of such therapy. Intracranial pressure monitoring is generally indicated in patients with severe head injury (GCS<8) who remain comatose. Institutional variability exists in methods for measurement, as do specific indications for monitoring. Elevation of the head of the bed to 30° will reduce ICP modestly without altering CPP. Mannitol (0.5–1.0 g/kg IV) may produce a short-term reduction in ICP. Mannitol causes an osmotic dehydration which is non-selective. Complications of mannitol therapy include fluid overload, hyperosmolality, hypovolaemia and rebound cerebral oedema. Mannitol may be used as a temporizing measure to enable a patient with a surgically remediable lesion to get to theatre. Routine use of hyperventilation in head injury is contraindicated. Hypocarbia reduces cerebral blood flow (and ICP) through vasoconstriction which, if extreme, may reduce CPP to the point of exacerbation of secondary brain injury [31]. Anticonvulsant prophylaxis (phenytoin 15–18 mg/kg IV over 30–60 minutes) is indicated for the prevention of seizures within the first week after injury [32]. Seizures are managed acutely using standard therapies and guidelines (including benzodiazepines and phenytoin). The use of barbiturates, endotracheal intubation and mechanical ventilation may be indicated for status epilepticus or seizures that are refractory to therapy. Antibiotic prophylaxis is indicated for compound fractures. Tetanus immunoprophylaxis is given as part of routine wound care. Steroid therapy has had varied support but is not recommended [33]; in 2005, the CRASH collaborators reported conclusively that intravenous corticosteroids should not be used in the treatment of head injury [34]. There has been considerable interest and experimental endeavour with regard to cerebral protection and salvage therapies. To date, no benefit has been demonstrated in the administration of aminosteroids, amino acids or monoamine antagonists in patients with head injury [35–37] and the role of calcium channel blockers remains unclear [38]. More recent research demonstrated worse outcomes for patients with diffuse traumatic brain injury who had a decompressive craniectomy [39]. The role of hypothermia is controversial; while animal studies have shown a benefit, prospective studies have shown either harm or no harm [40,41]. In summary, general supportive therapy, including the maintenance of thermoregulation, hydration, pressure care and nutrition are the mainstays of therapy. There are two features of prime importance to resuscitation in patients suffering neurotrauma: With elevation of intracranial pressure and loss of autoregulation of cerebral circulation, relatively higher systemic blood pressures are required. The practice of minimal-volume resuscitation has no place in the patient with serious neurotrauma. Standard approaches to the management of hypovolaemia in head- injured patients should be adopted. The use of hypertonic solutions in resuscitation (including hypertonic saline) has been studied with variable conclusions [42]. But the only randomized controlled trial performed with hypertonic saline showed no improvement in outcome [43]. Albumin has also been shown to have detrimental effects in severe traumatic brain injury [44]. Indications for intubation and ventilation of the neurotrauma patient are inadequate ventilation or gas exchange (hypercarbia, hypoxia, apnoea); inability to maintain airway integrity (protective reflexes); a combative or agitated patient; and the need for transport where the status of the airway is potentially unstable (between hospitals, to CT, to angiography, etc.). In patients with minimal–mild head injury, recommendations with regard to a ‘safe’ period of observation, need for hospital admission or predictive value of injury mechanism are not consistent. Rural and isolated settings present logistic difficulties in the management of this group. Careful observation for a prolonged period is a reasonable alternative and early neurosurgical consultation, together with a low threshold to transfer to a neurosurgical centre, is prudent. Patients with moderate to severe neurotrauma require hospital admission, preferably under the care of a neurosurgeon in a specialized neurosurgical unit or ICU. Rehabilitation and social readjustment is a focus of therapy from early in the clinical course. Inter-hospital transfer of patients with significant neurotrauma requires the attendance of skilled transfer staff and the maintenance of level of care during transfer. Airway management must anticipate the potential for the patient to deteriorate en route. The presence of pneumocephalus precludes unpressurized (high) altitude flight. The use of teleradiology and neurosurgical consultation will be of value in the management of the remote head-injured patient. The level of residual neurological impairment is a function of the severity of the degree of trauma and quality of care. A poor outcome is associated with prolonged pre-hospital time, delay of transfer to the appropriate facility, admission to an inappropriate facility and delay in definitive surgical treatment. Overall mortality in severe head injury is of the order of 35%. A lower GCS at presentation is associated with a worse outcome. Approximately half the patients who remain comatose with GCS<9 for longer than 6 hours will die [12]. Acute subdural haematoma and diffuse axonal injury producing persistent coma are associated with the vast majority of neurotrauma deaths. Early neurological abnormalities are, however, not reliable prognostic factors and an initial period of maximally aggressive therapy is indicated in patients with closed neurotrauma. Controversies
Trauma
3.1 Trauma overview
Epidemiology
The trauma system – background
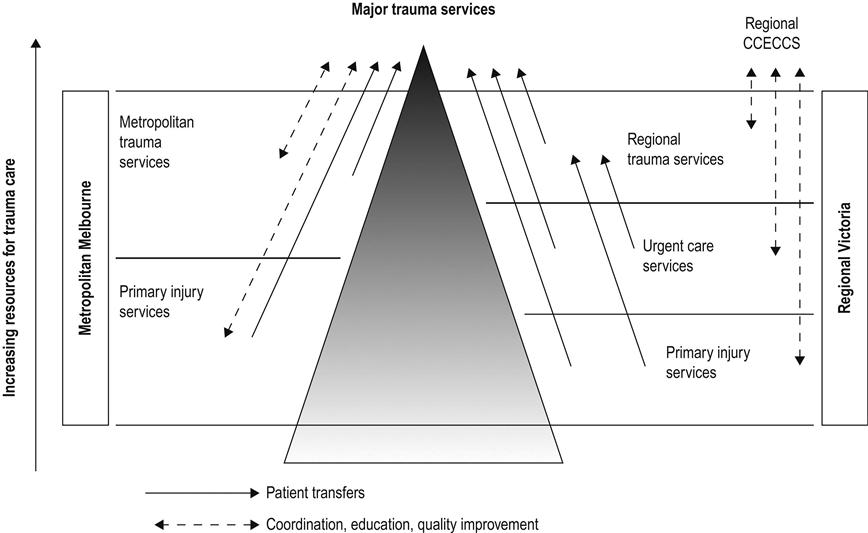
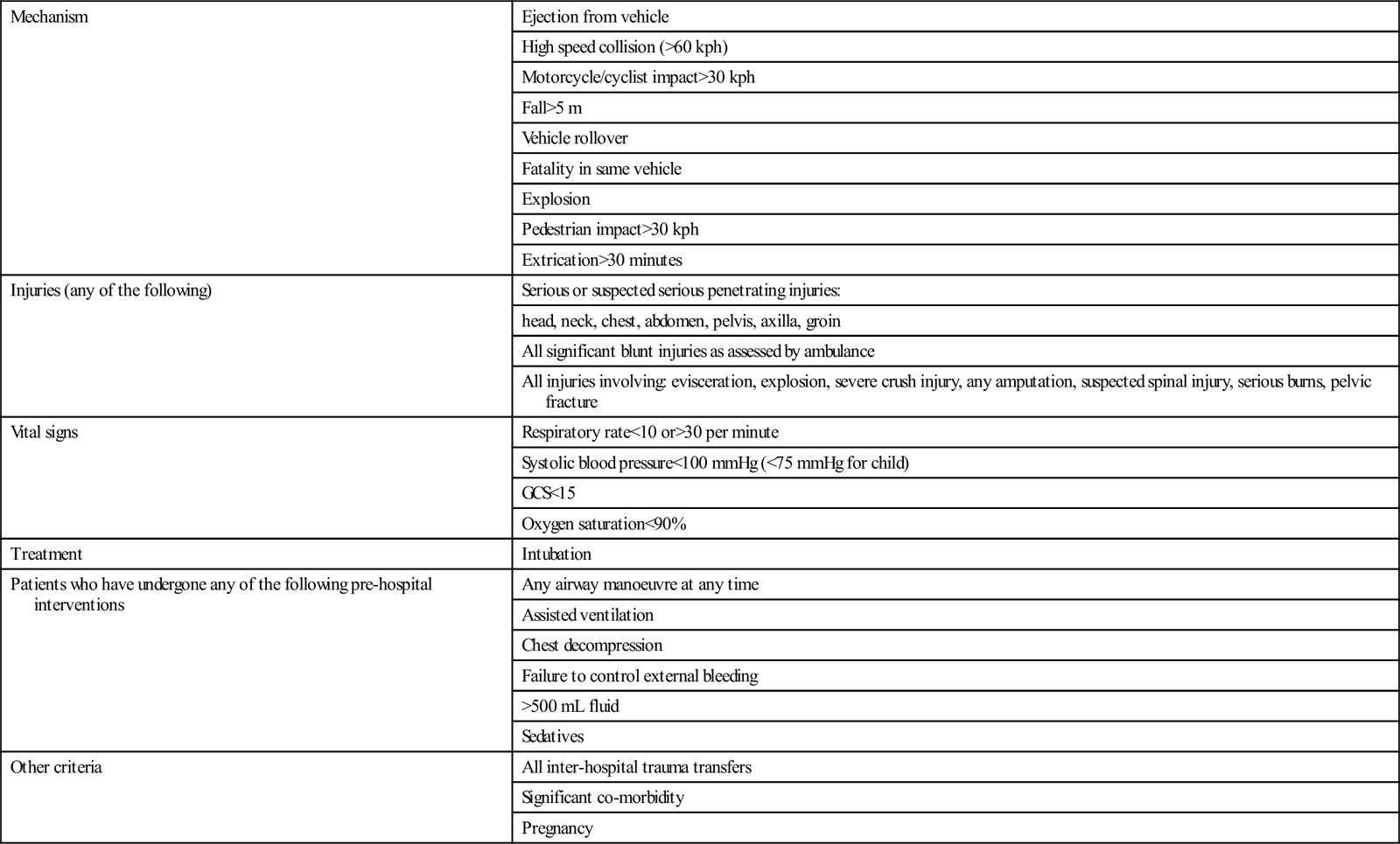
The trauma system – pre-hospital
Mechanism
Ejection from vehicle
High speed collision (>60 kph)
Motorcycle/cyclist impact>30 kph
Fall>5 m
Vehicle rollover
Fatality in same vehicle
Explosion
Pedestrian impact>30 kph
Extrication>30 minutes
Injuries (any of the following)
Serious or suspected serious penetrating injuries:
head, neck, chest, abdomen, pelvis, axilla, groin
All significant blunt injuries as assessed by ambulance
All injuries involving: evisceration, explosion, severe crush injury, any amputation, suspected spinal injury, serious burns, pelvic fracture
Vital signs
Respiratory rate<10 or>30 per minute
Systolic blood pressure<100 mmHg (<75 mmHg for child)
GCS<15
Oxygen saturation<90%
Treatment
Intubation
Patients who have undergone any of the following pre-hospital interventions
Any airway manoeuvre at any time
Assisted ventilation
Chest decompression
Failure to control external bleeding
>500 mL fluid
Sedatives
Other criteria
All inter-hospital trauma transfers
Significant co-morbidity
Pregnancy
The trauma system – intrahospital
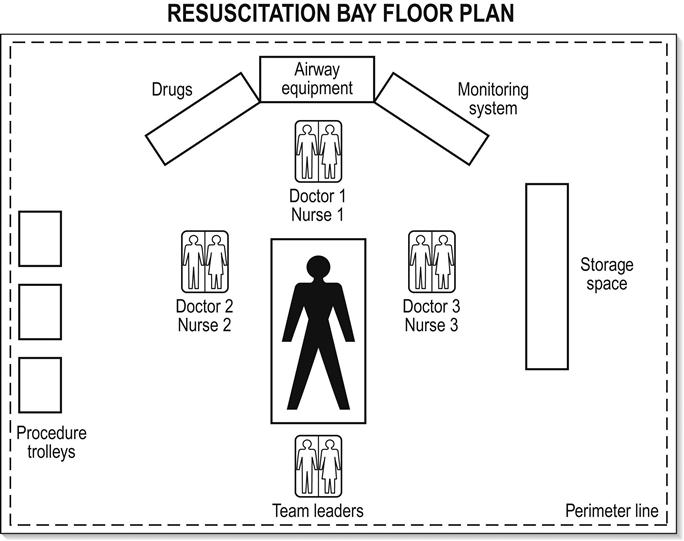
Preparation
Initial management
Airway
Breathing
Circulation
 Tension pneumothorax. This will cause rapid and severe disruption to the circulation.
Tension pneumothorax. This will cause rapid and severe disruption to the circulation.
 Anaphylactic shock and septic shock may coexist with hypovolaemic shock.
Anaphylactic shock and septic shock may coexist with hypovolaemic shock.
Disability
Exposure
Next steps
Trauma audit
Trauma in developing countries
3.2 Neurotrauma
Introduction
Pathogenesis

Classification of primary injury in neurotrauma
Skull fracture
Concussion
Contusion
Intracranial haematoma
Extradural
Subdural
Intracerebral
Subarachnoid and intraventricular haemorrhage
Diffuse axonal injury
Penetrating injury
Epidemiology
Prevention
Clinical features
Definition
History
Primary survey
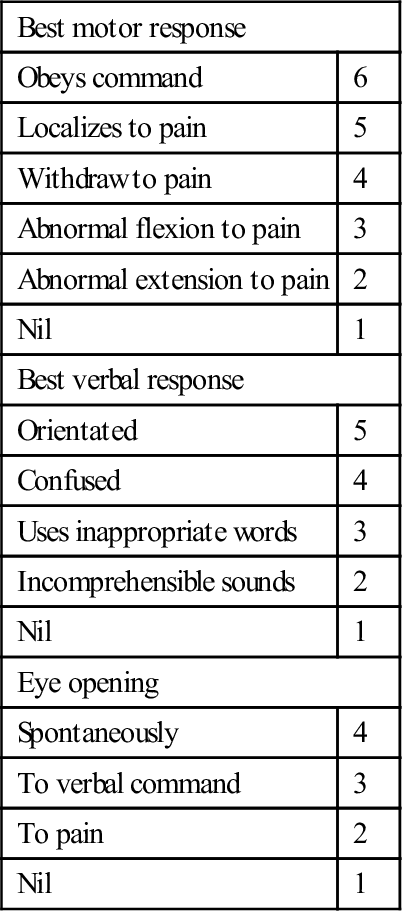
Secondary survey
 Fail to show eye opening in response to pain (eye-opening response=1)
Fail to show eye opening in response to pain (eye-opening response=1)
 Fail to obey commands (best motor response=5)
Fail to obey commands (best motor response=5)
 Make at best only incomprehensible sounds (best verbal response=2).
Make at best only incomprehensible sounds (best verbal response=2).
Best motor response
Obeys command
6
Localizes to pain
5
Withdraw to pain
4
Abnormal flexion to pain
3
Abnormal extension to pain
2
Nil
1
Best verbal response
Orientated
5
Confused
4
Uses inappropriate words
3
Incomprehensible sounds
2
Nil
1
Eye opening
Spontaneously
4
To verbal command
3
To pain
2
Nil
1
Clinical investigations
Minimal–mild head injury
Moderate–severe head injury
Treatment
Minimal–mild head injury
 Rest comfortably at home in the company of a responsible adult for the next 12–24 hours
Rest comfortably at home in the company of a responsible adult for the next 12–24 hours
 Resume normal activity after feeling recovered
Resume normal activity after feeling recovered
 Mild pain killers (such as paracetamol) may be taken for headache as directed by the doctor
Mild pain killers (such as paracetamol) may be taken for headache as directed by the doctor
 Avoid exposure to activities that may create risk of further head injury within the next 2 weeks
Avoid exposure to activities that may create risk of further head injury within the next 2 weeks
 If you require a certificate for work please make this clear to emergency department staff
If you require a certificate for work please make this clear to emergency department staff
Moderate–severe head injury
Resuscitation in neurotrauma
Disposition
Prognosis
< div class='tao-gold-member'>
Related posts:
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


3. Trauma