CASE 29
Incident
Clinical information:
• GCS 12 (E3, M5, V4).
• P 134.
• BP 90/55 mmHg.
• RR 9.
• SaO2 99% on mask oxygen.
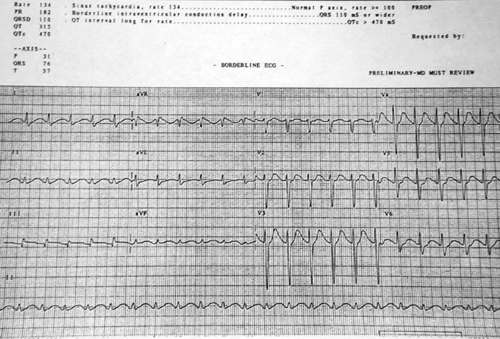
The attending doctor has faxed through an ECG to the PHR team. This poor-quality fax is pictured below.
 |
Relevant information
Questions
29.1 What additional information is relevant and how might the retrieval coordinator obtain this?
A close friend of the patient has since arrived at the hospital. He has found a large number of empty medication containers at the patient’s house. These included her usual tricyclic antidepressant and the previously dispensed analgesics.
29.2 What pre-retrieval advice should be given to the referral hospital medical staff?
On arrival, the Emergency Department is busy. The local medical team gives you a brief handover including their observation that the patient has been ‘stable’. They then excuse themselves and leave. Soon after, the patient has a generalised seizure.
29.3 Outline your response.
Discussion
29.1 Until proven otherwise, this patient has taken a life-threatening polypharmacy overdose. The analgesics alone do not explain the depressed conscious state and cardiac disturbance identified in the ECG. There is a sinus tachycardia and prolongation of the QRS and QT intervals. In addition, there is a right-ward axis with a terminal R wave in aVR. These findings, in combination with her requirement for mental health support should immediately raise the suspicion of tricyclic antidepressant (TCA) toxicity. Note that the degree of ECG abnormality following TCA ingestion reflects the risk of developing potentially lethal cardiac and neurological disturbances.
ECGs sent by fax are notoriously poor quality. The team should interpret it as best they can and discuss further with the local team.
It is highly likely that a large amount of paracetamol (and codeine phosphate) has also been ingested. This should not be overlooked when faced with the more acute concerns relating to the TCA effects.
Relevant information when coordinating a retrieval response can be considered as either critical (‘need to know’) or important (‘nice to know’). Critical information will usually impact upon the immediate actions required to both support this patient in her current location and mobilise a PHR team to retrieve her.
Critical information
• Which medications she has ingested (both type and quantity).
• Her access to any other medications.
• Likely time(s) of ingestion.
• Availability of medical staff with anaesthetic skills at the referring hospital.
• Availability of potential therapeutic agents at the referring hospital:
• N-acetylcysteine (NAC).
• Sodium bicarbonate and/or hypertonic saline.
• Naloxone.
• Availability of the PHR team and aircraft.
• Bed availability at receiving ICU.
Important information
Past medical history
• Factors that might increase her risk of liver injury following paracetamol overdose:
• Chronic alcohol abuse.
• Hepatic microsomal-inducing drugs (e.g. carbamazepine).
• Potential glutathione depletion (e.g. malnutrition).
• Pathological causes of liver injury such as viral hepatitis.
• Sustained release, chronic or repeated supratherapeutic paracetamol ingestion will alter the ongoing toxicology management.
Other relevant comorbidities
• Heart disease
• May increase risk of developing TCA-related cardiac complications and limit tolerance to large fluid volumes and sodium loads.
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


