CASE 25




Incident
The PHR team are tasked to a rural clinic to retrieve a 35-year-old female patient who presented 2 hours earlier with traumatic closed-head injury and quickly became unconscious. The local doctor has stabilised the patient and reports the following clinical information:
• Intubated and ventilated.
• Evidence of aspiration during intubation.
• SBP 90 mmHg.
• Single intravenous access (18-gauge cannula) obtained with difficulty.
Question
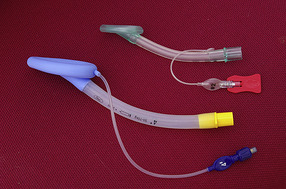
25.1 Describe each of the items of equipment shown and their use in the general pre-hospital and retrieval environment. Focus on the broad applications of the equipment, not the specific brand or make. Where relevant, comment on the use of this equipment in this scenario.
Discussion
‘Parapac’ portable ventilator
There are several areas of discussion concerning ventilators in the pre-hospital and retrieval environment and the focus here is on complex versus simple ventilators.
One approach is to keep the ventilator as simple as possible, particularly in the relatively uncontrolled pre-hospital and retrieval environment, in which other issues may be distracting the user. With this in mind, many services have opted for simple gas-powered ventilators as pictured. There is no battery to charge and one simple pressure dial to read. The user can set a rate and a tidal volume and there are visual aids to prompt for paediatric settings. There is a demand switch (essentially to start ventilating), a visual aid to confirm oxygen is available and a variable upper pressure limit. Audio alarms are also a feature. A final switch allows either 45% or 100% oxygen. Positive end expiratory pressure (PEEP) is added to the external circuit. Such a straightforward set-up reduces the chance of error and is of particular benefit to services that transfer ventilated patients infrequently or who have a high staff turnover rate within the PHR team.
The basic nature of such a ventilator can also be a downside. Complex patients, such as transfers between ICUs, very young children, asthmatics or patients with acute lung injury are hard to ventilate adequately on such a device. In addition, the ability to perform non-invasive ventilation (NIV) in the retrieval environment (see Case 39) depends on a reasonably sophisticated ventilator. If a retrieval service is to provide continuity and the same level of care during the transfer, it is hard to justify such a basic ventilator. With the importance of low tidal volume ventilation widely recognised in the management of ventilated patients, is it acceptable to use a ventilator with such limited ability to control tidal volumes? Whichever decision is made, the team must be comfortable with the use (and limitations) of the ventilator provided.
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


