Edited by Anthony Brown Stephen A Bernard Assessment and management of the airway is the first step in the resuscitation of a critically ill patient in the emergency department (ED). Once the airway has been assessed and managed, evaluation of adequacy of ventilation follows. This chapter outlines the initial management of airway and ventilation in the ED. Evaluation of the airway commences with a ‘look, listen, feel’ approach to detect partial or complete airway obstruction. If airway compromise is suspected, initial basic airway manoeuvres include the jaw thrust, chin lift and head tilt (providing with the latter that there is no suspicion of cervical spine injury); and placement of an oropharyngeal airway (OPA) (see Chapter 1.1 on Basic Life Support). Gentle direct inspection of the upper airway using a laryngoscope may be necessary to detect a foreign body, which can be removed using a Yankauer suction catheter for liquids/secretions and/or Magill’s forceps for solid material. Once the airway is cleared, supplemental oxygen by face-mask is commenced as consideration is given to the breathing status. Evaluation of breathing also uses a ‘look, listen, feel’ approach. Confirmation of adequate oxygenation initially uses a pulse oximeter. The adequacy of breathing may be confirmed with an arterial or venous blood gas analysis to confirm that the PCO2 is in the normal range. Conscious patients with a patent airway but who have hypoxia and/or hypercapnoea should then be considered for non-invasive ventilation (NIV) or endotracheal intubation (ETI) and mechanical ventilation. Many patients in respiratory failure with hypoxaemia and/or hypercapnoea may benefit from a trial of NIV [1]. The use of NIV involves administration of a controlled mixture of oxygen and air delivered at a set positive pressure via a tightly sealed face-mask. The pressure is generally maintained between 5 and 10 cm H2O during both inspiration and expiration. This continuous positive airway pressure (CPAP) recruits lung alveoli that were previously closed, improving the ventilation/perfusion ratio and thus helping to correct hypoxaemia. There may also be a reduction in the work of breathing as a result of an increase in pulmonary compliance. Inspiratory support (i.e. 5–20 cm H2O above the baseline pressure) during NIV is known as bi-level NIV. This additional inspiratory support is thought to further reduce the work of breathing when there is poor lung compliance or increased airway resistance. Contraindications to NIV include comatose or combative patients, poor tolerance of a tight-fitting face-mask, poor seal of the face-mask due to facial hair, and/or the lack of trained medical or nursing staff to institute and monitor the NIV. Patients who present with severe acute pulmonary oedema (APO) should receive CPAP to improve cardiac and pulmonary function, while medical therapy with nitrates and diuretics is initiated [2]. On the other hand, patients who present with an exacerbation of chronic obstructive pulmonary disease (COPD) may benefit from bi-level NIV rather than CPAP alone [3]. There is also some evidence to support the use of NIV in patients with respiratory failure due to other common ED conditions, such as community-acquired pneumonia [1], although the role of NIV in the management of asthma remains uncertain [4]. Thus, it is common ED practice to administer a trial of NIV in most awake patients with respiratory distress or respiratory failure, prior to any consideration of a requirement for ETI and mechanical ventilation. Endotracheal intubation (ETI) is performed for any one or more of the following four major reasons: to create an airway; to maintain an airway; to protect an airway; and/or to provide for mechanical ventilation. Thus, a patient in respiratory arrest requires immediate bag/valve/mask (BVM) ventilation with supplemental oxygen while preparation is made for ETI and mechanical ventilation to protect and maintain the airway and provide mechanical ventilation. Alternatively, a patient with a reduced conscious state and/or depression of the cough reflex requires ETI for airway maintenance and protection. Also, ETI may be indicated as part of general anaesthesia in the combative patient who needs imaging and/or a practical procedure. Finally, ETI will be required for mechanical ventilation in a patient with respiratory failure in whom NIV has been unsuccessful or is contraindicated. There are additional challenges to ETI in the ED compared to ETI in the operating theatre. There is often inadequate time for consultation with the patient and/or family and details of current medications, previous anaesthetics and/or allergies may not be available. Also, the status of the cervical spine in a patient with an altered conscious state following trauma is unknown, even if initial plain imaging appears normal. Finally, patients who present to the ED are generally not fasted and thus at a higher risk of aspiration of stomach contents during ETI. Given these risks, accreditation by the hospital for a medical practitioner to undertake ETI in the ED is essential. Such accreditation should be based on gaining appropriate qualifications as well as considerable experience in both the operating theatre or in the emergency department, under the supervision of an experienced anaesthetist or airway operator. In addition to initial accreditation, on-going skills maintenance in airway techniques using simulation training should be required [5]. A number of possible techniques for ETI in the ED are reviewed below. The selection of the appropriate technique depends upon physician preference and the clinical setting. A checklist approach is now becoming standard. Unless the patient is deeply comatose but not in cardiac arrest, upper airway reflexes will generally be present and ETI will require the use of sedative and neuromuscular blocking drugs to facilitate laryngoscopy and the placement of the endotracheal tube. Rapid sequence intubation (RSI) involves the simultaneous administration of sedative drugs and a rapid-onset muscle relaxant at a predetermined dose and is the technique of choice when intubation is required in the ED. Precautions and relative contraindications to the performance of RSI aim to avoid the technique in those judged to be difficult or impossible to intubate, including a patient with upper airway obstruction, distorted facial anatomy, micrognathia or an ankylosed neck. An alternative elective intubation technique in such cases may be awake intubation under local anaesthesia or an awake surgical airway (see later) to avoid at all costs creating the situation of ‘can’t intubate, can’t ventilate’. Careful preparation is essential prior to RSI. If time and patient status allow, seek a history of current medications, allergies and time of the last meal. Make a careful examination of the upper airway looking for anatomical features that may predict difficult intubation. A ‘4×4’ checklist to ensure adequate preparation prior to RSI is shown in Box 2.1.1. The conscious patient should receive explanation and reassurance during the preparatory phase. Pre-oxygenation with 100% oxygen is essential to prevent oxygen desaturation during the procedure. Ideally, NIV with 100% oxygen for a 3-minute period should be administered. If this is not possible, then spontaneous breathing through a tight-fitting bag/valve/mask using 15 L/min oxygen is an alternative way to pre-oxygenate the patient. In addition, the application of nasal prongs with continuous oxygen flowing at 15 L/min can decrease the incidence of hypoxia during the RSI process [6]. If the patient has suspected spinal column injury, the neck must be immobilized in the anatomically neutral position. Reliable intravenous access as well as equipment for suctioning the airway must be available as well as a tipping trolley. Monitoring required during RSI must include a continuous ECG trace and pulse oximetry. The blood pressure should be measured either non-invasively using an automated monitoring device each minute or invasively using an intra-arterial catheter. Waveform capnography for end-tidal carbon dioxide (ETCO2) measurement following RSI must be calibrated and ready to use. In addition, a disposable calorimetric capnograph should be available in case the waveform capnograph fails. The drugs required will depend on physician preference and the clinical situation. Common choices for induction include propofol at 1–2 mg/kg, a narcotic, such as fentanyl 1.0 μg/kg, a benzodiazepine, such as midazolam 0.05–0.1 mg/kg, followed by a rapid-onset depolarizing neuromuscular blocking drug, such as suxamethonium 1.5 mg/kg. Contraindications to suxamethonium include known allergy, hyperkalaemia, burns, crush injury, spinal cord injury (not in the acute setting) or a history of malignant hyperthermia. Therefore, an alternative when suxamethonium is contraindicated is the rapid acting non- depolarizing drug rocuronium 1 mg/kg [7]. Details of the indications, dosages and side effects of all the commonly used drugs for RSI intubation are shown in Table 2.1.1. Table 2.1.1 Common intravenous drugs for rapid sequence intubation All drugs must be drawn up and checked in advance and the syringes clearly labelled. A spare laryngoscope must be available in case of failure of the first and the appropriate size of endotracheal tube (ETT) opened, lubricated and the cuff checked. Another ETT (one size smaller) should be immediately available. Finally, a bougie must be ready to hand. An ETT introducer (stylet) is preferred by some to provide a ‘hockey-stick’ J-shape to the end of the ETT. At least two assistants will be required; one to assist the operator with the drugs and equipment and another to provide cricoid pressure following the administration of sedation and muscle relaxation drugs. If cricoid pressure is utilized, it must not allow distortion or impediment to the visualization of the vocal cords; if this occurs, it may be abandoned to improve and optimize the laryngoscopic view. A fourth person is required to provide in-line manual immobilization in the case of RSI for the trauma patient with possible spinal column injury. Additional equipment in case of difficult or failed intubation should be readily available, ideally kept together in the ‘Airway Trolley’ containing the items necessary for a failed intubation protocol as shown in Figure 2.1.1. When all preparations are complete, including pre-oxygenation, the sedative drugs are administered as a bolus with gentle cricoid pressure applied via the cricoid ring cartilage. As consciousness is lost, the muscle relaxant is administered. Following fasciculations and the loss of muscle tone, firm cricoid pressure is applied and laryngoscopy performed. The patient is positioned in the ‘sniffing the morning air’ position with the neck flexed and the head extended, using a pillow under the head. The laryngoscope is inserted and the vocal cords visualized. If the larynx is sighted, the endotracheal tube is placed directly through the vocal cords into the trachea, the cuff inflated and the ETT secured with tapes. Many brands of ETT now include a line marked proximal to the cuff which should be visible at the conclusion of laryngoscopy, thus avoiding placement of the ETT in the right main bronchus. Cricoid pressure should be maintained until the position of the tube is checked with the waveform capnograph and the ETT secured. The operator then indicates that the ETT is correctly placed and cricoid pressure may be released. Clinical methods of ensuring optimal tracheal position include sighting the passage of the ETT through the vocal cords, misting of the ETT during exhalation and auscultation of breath sounds in both the lung fields. However, these clinical tests may be misleading and, in all cases, the ETT must be confirmed as placed in the trachea using waveform capnography, which is the gold standard for confirmation of tracheal placement in patients with a palpable pulse. However, during cardiac arrest there may be inadequate delivery of carbon dioxide to the lungs and hence a false-negative reading. In this setting, any doubt about correct airway placement should include removal of the ETT and ventilation using a supraglottic airway [8]. After placement of the ETI is confirmed, an orogastric or nasogastric tube should be inserted and a chest X-ray (CXR) performed to confirm correct positioning of the tip of the ETT in the trachea at least 1 cm proximal to the tracheal carina. The CXR also allows confirmation of correct placement of the orogastric or nasogastric tube in the stomach. As the drugs used for sedation and muscle relaxation wear off, further drugs for the maintenance of sedation and paralysis will be required. Appropriate monitoring of vital signs, pulse oximetry and waveform capnography with visual and audible alarms must be maintained at all times. Humidification of the inspired oxygen is desirable using a disposable heat and moisture exchange filter. When the patient is placed on mechanical ventilation, the PaCO2 should be checked to ensure adequate ventilation and to confirm correlation with the ETCO2. The unconscious patient also requires eye care, pressure area care, temperature control and catheterization of the urinary bladder. Hypotension following endotracheal intubation is common and must be addressed promptly. The causes include the vasodilator and/or negative inotropic effects of the sedative drug(s) given and/or the reduction in preload from positive-pressure ventilation decreasing venous return and cardiac output. Treatment consists of administration of a 10–20 mL/kg fluid bolus of crystalloid fluid, such as saline or Hartmann’s and/or infusion of a vasopressor/inotrope, de- pending on the clinical setting. Alternatively, in the setting of bronchospasm, hypotension may be due to gas trapping and dynamic hyperinflation from excessive ventilation, with the development of auto-PEEP (positive end-expiratory pressure), which is improved by immediate reduction in ventilation and allowing increased time for expiration. Importantly, hypotension can be due to the development of a tension pneumothorax occurring after the commencement of positive-pressure ventilation. On the other hand, hypertension usually indicates inadequate sedation and should be treated with supplemental sedation. The following additional measures need to be considered during intubation in patients with severe head injury. An assistant must hold the head in the neutral position due to the possibility of cervical spine instability, which increases the difficulty of visualizing the larynx. Laryngoscopy may raise intracranial pressure, although the benefit of pretreatment with lignocaine 1.5 mg/kg is uncertain in this setting [9]. In addition, thiopentone or propofol must be used cautiously in patients with severe head injury as profound hypotension due to unrecognized hypovolaemia may occur. In this setting, ketamine may be the preferred induction agent since this agent is more likely to maintain blood pressure compared with other sedating agents [10]. The technique of RSI is not recommended for a patient with a grossly abnormal upper airway and/or impending upper airway obstruction. In this setting, the larynx may then not be able to be visualized and ventilation of the now apnoeic patient may become impossible, leading to the ‘can’t intubate, can’t ventilate’ situation. An awake technique using local anaesthesia and/or a fibreoptic-assisted intubation should be performed in these patients (see later). Alternatively, an inhalational anaesthetic agent or a short-acting intravenous agent, such as propofol, can be used, as the sedative effects will rapidly reverse and spontaneous respirations resume if intubation and ventilation prove impossible. Endotracheal intubation under direct vision may be easy or difficult, depending on the view of the larynx during laryngoscopy. This laryngeal view has been classified by Cormack and Lehane into grades 1–4 [11]. A Cormack and Lehane grade 1 laryngoscopy is a clear view of the entire laryngeal aperture. A grade 2 laryngoscopy is a view of only the posterior part of the larynx. In a grade 3 laryngoscopy, only the epiglottis is visualized and in grade 4 only the soft palate is seen. A difficult intubation is defined as a Cormack and Lehane grade 3 or 4 view at laryngoscopy. Difficult intubation may be anticipated in the presence of pathological facial and upper airway disorders that may be congenital or acquired, such as maxillofacial and airway trauma, airway tumour or abscess or cervical spine immobility. There may also be anatomical reasons for a Cormack and Lehane grade 3–4 laryngoscopy, such as micrognathia or microstomia, poor mouth opening and/or a large tongue. A range of clinical tests have been proposed that help predict difficulty in visualization of the larynx, including relative size of the tongue to the pharynx, atlanto- occipital joint mobility and a thyromental distance<6 cm. However, these are not always clinically useful in the emergency setting. More recently, sonographic measurements of anterior neck soft tissue thickness at the level of hyoid bone and thyrohyoid membrane have been used to distinguish difficult and easy laryngoscopy [12]. Attempts at blind placement of the ETT into the trachea when the larynx is not visualized are unlikely to be successful and may result in pharyngeal or laryngeal trauma making the situation even more difficult, with hypoxaemia. In this situation, a failed intubation drill must be immediately initiated [13]. A failed intubation algorithm suitable for use in the ED is shown in Figure 2.1.1. The first step is to ensure that all medical and nursing staff present are made aware that the intubation is difficult and that a failed intubation drill is being initiated [14]. Second, depending on hospital resources, an urgent call for assistance from another physician with additional experience should be made. Simple initial manoeuvres to improve visualization of the larynx include adding a second pillow to flex the neck further (unless cervical spine injury is suspected), the use of a straight Mackintosh laryngoscope blade and ‘backward/upward/rightward external pressure’ (BURP) on the thyroid cartilage with abandonment of cricoid pressure if needed. If the larynx still cannot be visualized, blind placement of a bougie and subsequent railroading of a well lubricated size 7.0 mm ETT over the bougie should be attempted [15]. Correct bougie airway placement is suggested by feeling the tracheal rings ‘clicks’ and by hold-up at around 30–40 cm as the bougie reaches distally in a mainstem bronchus. Absence of hold-up indicates likely oesophageal placement. Rotating the ETT through 90° in an anticlockwise direction may be helpful to facilitate passage along the bougie through the larynx. If this initial step at ETI is unsuccessful, adequate oxygenation must be re-established and or maintained using a bag/mask with an OPA or a laryngeal mask airway (LMA) between attempts at intubation. If oxygenation is able to be maintained using bag/valve/mask ventilation, alternative approaches suitable for use in the ED should be considered. A summary of these approaches for a failed intubation is given in Figure 2.1.1. However, if oxygenation cannot be maintained during the drill, immediate cricothyroidotomy is indicated. The LMA is commonly used for airway management during elective general anaesthesia. During a failed intubation drill, the LMA may be superior to a bag/mask and oral airway for oxygenation and ventilation, even though there is still the potential risk of aspiration of the contents of the stomach into the airway as this remains unprotected. This risk may be decreased with the use of an LMA with a distal drainage tube (LMA ProSeal™) or an LMA incorporating an oesophageal vent that allows placement of an orogastric tube to provide access for suctioning the upper oesophagus (LMA Supreme™) [16]. In addition to the provision of oxygenation and ventilation, there are a number of modified LMAs that may be useful to facilitate intubation during a failed intubation drill in the ED. The intubating LMA is a modification of the standard LMA that incorporates a rigid curved outer airway tube with a metal handle and a special modified endotracheal tube specifically made to pass blindly through the LMA into the trachea (LMA Fastrach™). An LMA incorporating a video image of the larynx has been developed (LMA CTrach™), which may facilitate passage of a bougie through the LMA into the trachea. The LMA can then be removed and an ETT placed over the bougie. The latter has a higher success rate for first-time intubation compared with the LMA Fastrach [17]. There are an increasing number of laryngoscopes available that include a video image projected from the tip of the laryngoscope and displayed on a separate small screen or laryngoscopes with the screen fitted to the handle. These have the advantage of giving a superior view of the larynx and, although the first-pass success rate appears to be similar to traditional direct laryngoscopy [18]. Increasing familiarity may see this become the preferred method of laryngoscopy. A fibreoptic bronchoscope may assist in the intubation of the patient when RSI fails or is contraindicated. In particular, fibreoptic bronchoscope-assisted intubation (FBI) is the technique of choice in suspected traumatic injury to the larynx and in the obstructed airway, particularly with distorted anatomy, such as with an upper airway burn or tumour. The FBI may diagnose the severity of the laryngeal injury or pathology and the possible requirement for surgery. However, it requires considerable training and should only be performed by an experienced operator, usually in theatre. Equipment sterilization, maintenance and checking procedures must also be in place. Topical anaesthetic is applied to the nasal passage using gauze soaked in 5 mL of lignocaine 2% with adrenaline 1:100 000 if the patient is aware. In addition, the upper airway is anaesthetized with lignocaine 10% spray. A well-lubricated 7.0 mm ETT is introduced nasally and passed to the posterior pharynx. Then the bronchoscope is inserted through the ETT to visualize the vocal cords. The suction port of the bronchoscope is used to clear any secretions and also to administer further local anaesthesia into the airway. The bronchoscope is advanced through the larynx and the ETT then railroaded over the bronchoscope and down the trachea. Further sedation to decrease the cough reflex will be required at this time. The bronchoscope is removed and the patient is then ventilated with oxygen and given additional sedation as needed. If an LMA has been used during a failed intubation drill and is in place to provide ventilation, this may be utilized to guide the bronchoscope into the larynx. A guidewire may be passed via the bronchoscope into the trachea. The LMA is then removed and an ETT is replaced over the guidewire [19]. The use of a fibreoptic bronchoscope in the ED is limited by several factors. The bronchoscope and light source must be immediately available for a failed intubation drill. The technique requires considerable additional practice for skills maintenance, yet its use is rare in routine ED practice. The larynx may be difficult to visualize in the presence of blood, vomitus or secretions. Finally, the equipment is expensive to purchase and maintain. If the patient is able to be adequately oxygenated with a supraglottic airway, the technique of retrograde intubation may be used in the ED [20]. The cricothyroid membrane is punctured by a needle and a guidewire is passed and directed cephalad. The wire is then brought out through the mouth using Magill’s forceps. The ETT may be passed over the wire and back into the larynx using the introducer of a cricothyroidotomy kit [21]. Alternatively, the wire may be passed inside the end of the ETT and then out through the ‘Murphy eye’. Resistance may be felt when the ETT reaches the larynx and some anticlockwise rotation may be required to facilitate passage into the larynx. When the level of the cricothyroid is reached, the guidewire is removed and the ETT passed further down the trachea. The technique of retrograde intubation takes time and experience to perform and is usually unsuitable in a critical airway emergency. Blind nasotracheal intubation (BNTI) is a traditional technique that may still occasionally be useful in the ED, either as the initial technique of choice or as part of a failed intubation drill once spontaneous respirations have resumed [22]. Contraindications include a fractured base of skull or maxillary fracture, a suspected laryngeal injury, coagulopathy and/or upper airway obstruction. High-flow oxygen is administered by mask and the nasal passages are inspected to assess patency. The larger nasal passage is prepared as per the nasal fibreoptic intubation described above. Local anaesthetic may also be sprayed into the upper airway and intravenous sedation may be administered if required and clinically appropriate. An ETT one size smaller than the predicted oral size is passed via the nose to the pharynx and advanced slowly towards the larynx with the operator listening for breath sounds. The head may need to be flexed, extended or rotated to facilitate entry into the larynx, the ETT rotated clockwise through 90° and/or a suction catheter used to guide the ETT. When the tube passes into the trachea, louder spontaneous respirations heard from the ETT or the onset of coughing down the tube, confirm successful placement. However, there are significant complications with BNTI including epistaxis, injuries to the turbinates, perforation of the posterior pharynx, laryngospasm and injury to the larynx. Cricothyroidotomy is an essential skill for all emergency physicians and must be considered immediately in the situation of ‘can’t intubate, can’t ventilate’. There are several possible techniques for emergency cricothyroidotomy described below. Proprietary kits allow a cricothyroidotomy tube to be placed using a Seldinger technique. In this approach, the cricothyroid membrane is punctured with a needle mounted on a syringe; free aspiration of air confirms placement in the airway. A guidewire is passed through the needle caudad down the trachea. The needle is then removed and a dilator passed along the wire, then a 4.5–6 mm cricothyroidotomy tube is mounted on a guide and passed along the wire and into the trachea. The position of the cricothyroidotomy tube must be carefully checked as it is possible to misplace it anterior to the trachea. Note, if the cricothyroidotomy tube is uncuffed, interpretation of a capnograph waveform can be misleading as much of the exhaled gas passes into the upper airway and not out through the cricothyroidotomy tube during exhalation, resulting in a potentially false-negative end-tidal CO2 trace. Alternatively, a surgical cricothyroidotomy may be rapidly performed by making a small vertical incision over the cricothyroid membrane. Artery forceps are then used for blunt dissection to the cricothyroid membrane which is opened horizontally with the artery forceps. A bougie is passed through the opening into the trachea, then a size 6 mm cuffed ETT is ‘railroaded’ over the bougie. The ETT cuff is inflated, the bougie removed and bag/valve ventilation with oxygen commenced. This technique is faster to perform than a guide-wire technique, although physicians with limited surgical experience may prefer the guidewire approach [23]. Longer-term placement of a larger (>6 mm) ETT through the cricothyroid membrane is unsatisfactory because of the possibility of stricture occurring at the level of the cricoid ring. Therefore, the cricothyroidotomy is subsequently converted to either oral endotracheal intubation or a tracheostomy when it is safe and convenient to do so. Compared with cricothyroidotomy, a surgical tracheostomy is time-consuming and difficult to perform in the ED [24], but may be indicated in suspected direct laryngeal injury. Pre-tracheal dissection requires adequate lighting, instruments and diathermy, with distorted anatomy and bleeding making the technique more complex. Percutaneous dilatational tracheostomy is commonly performed in the ICU and can be rapidly performed by an experienced operator in the ED [25]. Once intubation has been achieved, the patient is connected to a mechanical ventilator to provide continued ventilatory support. Because ventilated patients can initially be managed for some time in the ED, it is important that recommendations for optimal mechanical ventilation are implemented in the ED. A tidal volume of 8 mL/kg and a respiratory rate of 10–14 breaths per minute are considered safe for most patients. In general, 5 cm of positive end-expiratory pressure (PEEP) is provided. However, patients with acute lung injury may have reduced pulmonary compliance and elevated peak inspiratory and plateau pressures. These patients should receive a ‘protective lung ventilation strategy’ [26]. This involves limiting the tidal volume to 6 mL/kg, with the respiratory rate setting increased to 16–20 breaths per minute to prevent excessive hypercapnoea. If hypoxia persists (PaO2<60 mmHg), then additional PEEP is indicated. This may be titrated in steps of 2.5 mmHg towards a maximum of 22 mmHg [27]. It is important to measure peak and plateau pressures in such a patient to avoid excessive intrinsic lung pressures. The latter is undertaken by pausing ventilation at end-inspiration for 10 seconds and observing the pressure trace on the screen of the ventilator. Patients with severe airways obstruction, such as asthma or COPD, should receive a standard tidal volume of 8 mL/kg, but at a decreased respiratory rate of 4 to 8 breaths per minute to allow sufficient time for adequate passive exhalation [28]. This slow respiratory rate reduces the risk of dynamic pulmonary hyperinflation and development of auto-PEEP leading to hypotension. Using this strategy, the PaCO2 level will rise (‘permissive hypercapnoea’) as oxygenation is maintained. In complete contrast, deliberate hyperventilation using a respiratory rate of 16–20 breaths per minute may be indicated to provide hypocapnoea in a patient who has been intubated and who has a severe metabolic acidosis, such as diabetic ketoacidosis. Also, hyperventilation in a patient with raised intracranial pressure to normocapnoea or slight hypocapnoea temporarily reduces the intracranial pressure while other treatments are being implemented. Increasingly, patients who are intubated pre-hospital by paramedics or by a physician in the ED may be considered for planned extubation in the ED, after investigation and treatment have excluded the requirement for mechanical ventilation in ICU. Examples include a patient with a drug overdose or those requiring brief general anaesthesia for a procedure. In general, patients should be lightly sedated with a short-acting sedative, such as propofol, able to follow commands and able to cough adequately to tracheal suction. Ideally, a trial of spontaneous breathing with the ventilator set to a CPAP of 5 cm H2O, with minimal inspiratory pressure support (i.e. 5–10 cm H2O) with modest supplemental oxygen (i.e.<50% oxygen) is necessary. Also, the stomach should be emptied via an orogastric or nasogastric tube prior to extubation. David R Smart Oxygen was first discovered by Priestley in 1772 and was first used therapeutically by Beddoes in 1794. It now forms one of the cornerstones of medical therapy. Oxygen (O2) constitutes 21% of dry air by volume. It is essential to life. Cellular hypoxia results from a deficiency of oxygen, regardless of aetiology. Hypoxaemia is a state of reduced oxygen carriage in the blood. Hypoxia leads to anaerobic metabolism that is inefficient and may lead to death if not corrected. A major priority in acute medical management is correction of hypoxia, hence oxygen is the most frequently administered and important drug in emergency medicine. There are sound physiological reasons for the use of supplemental oxygen in the management of acutely ill and injured patients. Oxygen proceeds from inspired air to the mitochondria via a number of steps known as the oxygen transport chain. These steps include: The normal partial pressure of inspired air oxygen (PIO2) is approximately 20 kPa (150 mmHg) at sea level. If there is a reduction in the fraction of inspired oxygen (FIO2), as occurs at altitude, hypoxia results. This is relevant in the transport of patients at 2400 m in commercial ‘pressurized’ aircraft, where ambient cabin pressures of 74.8 kPa (562 mmHg) results in a PIO2 of 14.4 kPa (108 mmHg). Hypoxia can result from inadequate delivery of inspired gas to the lung. The many causes include airway obstruction, respiratory muscle weakness, neurological disorders interfering with respiratory drive (seizures, head injury), disruption to chest mechanics (chest injury) or extrinsic disease interfering with ventilation (intra-abdominal pathology). These processes interfere with the maintenance of an adequate alveolar oxygen partial pressure (PAO2), which is approximately 13.7 kPa (103 mmHg) in a healthy individual. An approximation of the alveolar gas equation permits rapid calculation of the alveolar oxygen partial pressures: Oxygen diffuses across the alveoli and into pulmonary capillaries and carbon dioxide diffuses in the opposite direction. The process is passive, occurring down concentration gradients. Fick’s law summarizes the process of diffusion of gases through tissues: where In healthy persons, oxygen rapidly passes from the alveoli to the blood and, after 0.25 seconds, pulmonary capillary blood is almost fully saturated with oxygen, resulting in a systemic arterial oxygen partial pressure (PaO2) of approximately 13.3 kPa (100 mmHg). The difference between the PAO2 and the PaO2 is known as the alveolar to arterial oxygen gradient (A−a gradient). It is usually small and increases with age. The expected A−a gradient when breathing air approximates to: Age (years)÷4+4. An approximation of the actual value can be calculated as follows: There is a defect in pulmonary gas exchange if the calculated value exceeds the expected value. The A−a O2 gradient is increased if there is a barrier to diffusion, such as pulmonary fibrosis or oedema or a deficit in perfusion, such as a pulmonary embolism. An increased A−a gradient also reflects widespread ventilation–perfusion mismatch. In circumstances of impaired diffusion in the lung, raising the FIO2 assists oxygen transfer by creating a greater pressure gradient from the alveoli to the pulmonary capillary. The increase in FIO2 may not be as helpful when lung perfusion is impaired as a result of increased intrapulmonary shunting. Four steps are required to deliver oxygen to the periphery: The haemoglobin–oxygen (Hb–O2) dissociation curve is depicted in Figure 2.2.1, which also summarizes the factors that influence the position of the curve. If the curve is shifted to the left, this favours the affinity of haemoglobin for oxygen. These conditions are encountered when deoxygenated blood returns to the lung. A shift of the curve to the right favours unloading of oxygen and subsequent delivery to the tissues. A number of advantages are conferred by the shape of the Hb–O2 dissociation curve that favour uptake of oxygen in the lung and delivery to the tissues: Oxygen is carried in the blood as dissolved gas and in combination with haemoglobin. At sea level (101.3 kPa), breathing air (FIO2=0.21), the amount of oxygen dissolved in plasma is small (0.03 mL oxygen per litre of blood for each 1 mmHg PaO2). Hence at PaO2=100 mmHg, 3 mL of oxygen are dissolved in each litre of plasma. Dissolved oxygen is important because it is the first available oxygen to diffuse into the tissues. The dissolved component assumes greater significance in the hyperbaric environment, where at 284 kPa and FIO2=1.0 up to 60 mL oxygen can be carried dissolved per litre of blood. Haemoglobin carries 1.34–1.39 mL oxygen per gram when fully saturated. Blood with a haemoglobin concentration of 150 g/L carries approximately 200 mL oxygen per litre. The total amount of oxygen delivered to the body per minute is known as oxygen flux. where Hb=haemoglobin concentration g/L; SaO2=arterial oxygen saturation (percentage); PaO2=partial pressure of arterial oxygen (mmHg); Q=cardiac output (L/min). A healthy individual breathing air transports approximately 1000 mL of oxygen per minute to the tissues, based on a cardiac output of 5 L/min; 30% or 300 mL/min of this oxygen is not available, because at least 2.7 kPa (20 mmHg) driving pressure is required to allow oxygen to enter the mitochondria. Therefore, approximately 700 mL/min are available for use by peripheral tissues. This provides a considerable reserve above the 250 mL/min consumed by a healthy resting adult. In illness or injury, this reserve may be considerably eroded. Factors that reduce oxygen flux include a fall in cardiac output of any aetiology (including shock states), anaemia or a reduction in functional haemoglobin (carbon monoxide poisoning) and a drop in the SaO2. These situations are frequently encountered in the emergency department. Supplemental oxygen is required in addition to specific therapy, such as volume replacement, transfusion, and measures to improve cardiac output. Cellular hypoxia results if there is impairment of perfusion to local tissues. Oedema associated with medical illness or local injury increases the diffusion distance between blood and the cell, thus mandating a higher PaO2 to ensure adequate tissue oxygen delivery. Increased oxygen flux is required if: Elevation of cardiac output increases oxygen flux in these circumstances but, frequently, this too is significantly impaired by the disease state. Tissue demands for oxygen increase by 7% for each degree Celsius elevation in body temperature and considerably greater increases in demand occur in seizures, sepsis, severe dyspnoea, restlessness and shivering. Tissue extraction of oxygen is impaired in sepsis and by poisons, such as carbon monoxide or cyanide. In all cases, oxygen therapy must be combined with general measures, such as reduction of fever and specific treatment of the primary disease process. Oxygen delivery systems are classified into three groups (Box 2.2.1): These systems deliver a variable FIO2 to the patient which is altered by the inspiratory flow rate, the minute volume of the patient and the physical characteristics of the delivery system. These systems deliver a specified FIO2 to the patient that is not altered by changes in ventilatory pattern, volume or inspiratory flow rate. This is a subgroup of fixed-performance systems wherein 100% oxygen is delivered to the patient. The oxygen source in most Australasian emergency departments consists of a wall-mounted flow meter capable of delivering oxygen up to 15 L/min, with most available oxygen delivery systems connecting to this apparatus. A 15 L/min flow rate limits the delivery of high FIO2 to adults for the following reasons: Multiple-port oxygen supply outlets can overcome the above limitations of inspiratory flow rate and minute volume. The use of ‘Y’ connectors and ‘T’ pieces enable 30, 45 or 60 L per minute to be delivered to the patient to achieve an FIO2 of nearly 1.0, however, these systems can be untidy, using multiple hoses. More efficient control of flow is achieved via higher output or dial-up flow meters. Extra source oxygen flow may cause variable-performance systems such as the Hudson mask to become fixed-performance systems. Hence the terms ‘variable performance’ and ‘fixed performance’ are loosely applied and are largely dependent on whether or not the gas flow delivered is sufficient to match the patient’s ventilatory requirements. An example of this is in paediatric oxygen delivery. A high FIO2 can be delivered using a standard 15 L/min oxygen source because the child’s ventilatory requirements are smaller in proportion to the available oxygen supply. The oxygen delivery systems available for use in emergency medicine, summarized in Box 2.2.1, can be further subdivided according to economy of oxygen use and whether or not the system can be used to ventilate the patient manually. The FIO2 delivered by these systems is summarized in Table 2.2.1. Options available for use in emergency medicine include:
Critical Care
2.1 Airway and ventilation management
Introduction
Evaluation of the airway
Evaluation of breathing
Non-invasive ventilation
Clinical indications for non-invasive ventilation in the ED
Endotracheal intubation
Challenges to ETI in the emergency department
Accreditation in ETI
Rapid sequence intubation
Precautions and relative contraindications to RSI
Preparation for RSI
Pre-oxygenation
Monitoring during RSI
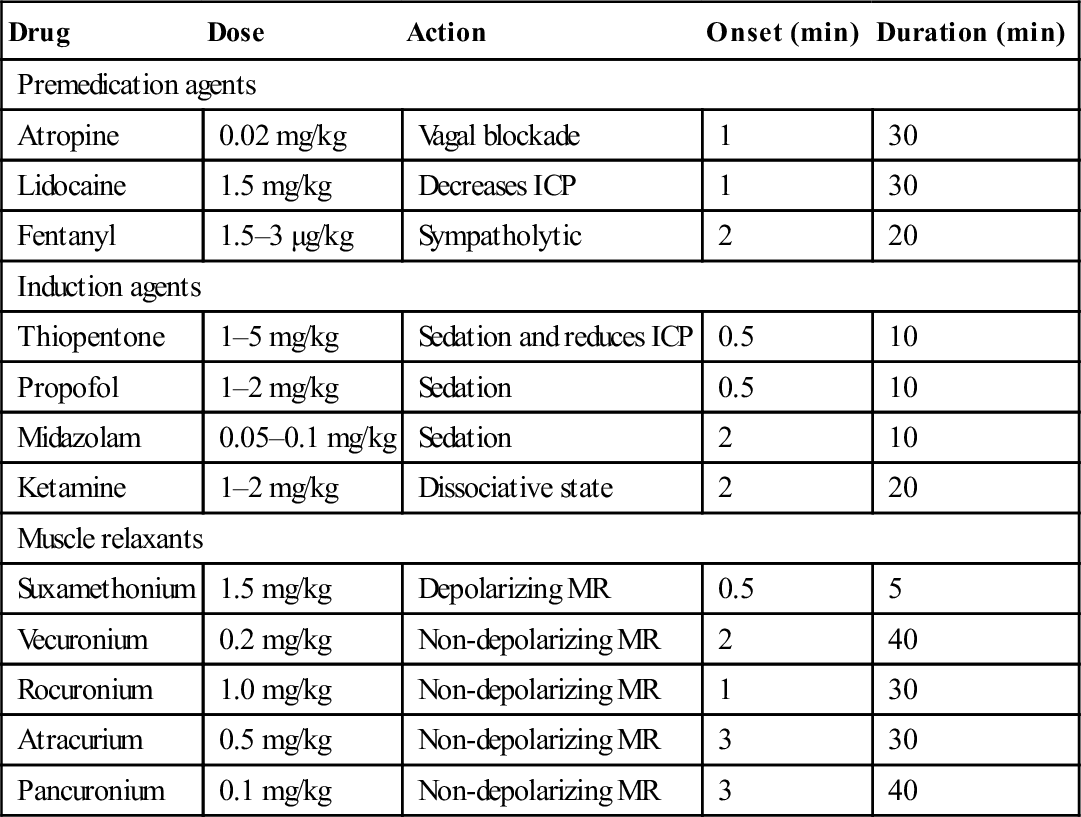
Drugs used in RSI
Drug
Dose
Action
Onset (min)
Duration (min)
Premedication agents
Atropine
0.02 mg/kg
Vagal blockade
1
30
Lidocaine
1.5 mg/kg
Decreases ICP
1
30
Fentanyl
1.5–3 μg/kg
Sympatholytic
2
20
Induction agents
Thiopentone
1–5 mg/kg
Sedation and reduces ICP
0.5
10
Propofol
1–2 mg/kg
Sedation
0.5
10
Midazolam
0.05–0.1 mg/kg
Sedation
2
10
Ketamine
1–2 mg/kg
Dissociative state
2
20
Muscle relaxants
Suxamethonium
1.5 mg/kg
Depolarizing MR
0.5
5
Vecuronium
0.2 mg/kg
Non-depolarizing MR
2
40
Rocuronium
1.0 mg/kg
Non-depolarizing MR
1
30
Atracurium
0.5 mg/kg
Non-depolarizing MR
3
30
Pancuronium
0.1 mg/kg
Non-depolarizing MR
3
40
Preparation of equipment and personnel prior to RSI
Endotracheal tube insertion
Ensuring optimal tracheal position
Maintenance of sedation and paralysis
Complications of RSI
Intubation in a patient with severe head injury
Difficult intubation
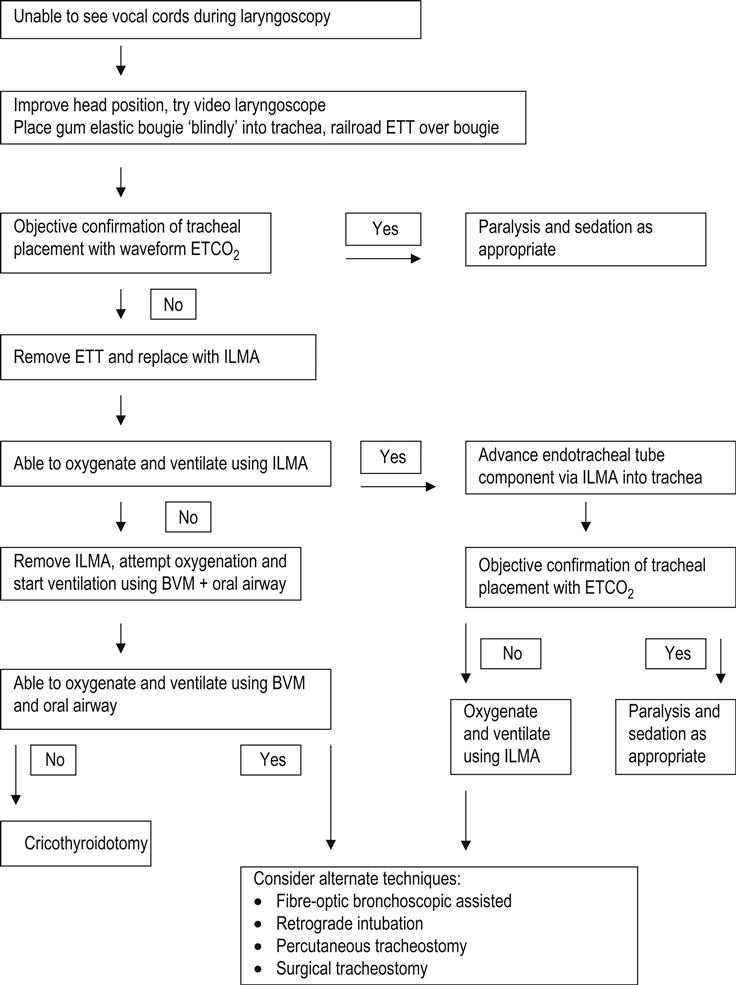
Failed intubation drill
Laryngeal mask airway
Modified laryngeal mask airways
Video-laryngoscope assisted intubation
Fibreoptic bronchoscope-assisted intubation
Technique of fibreoptic bronchoscope-assisted intubation
Limitations of fibreoptic bronchoscope-assisted intubation
Other airway management techniques
Retrograde intubation
Blind nasotracheal intubation
Technique of blind nasotracheal intubation
Cricothyroidotomy
Guidewire cricothyroidotomy
Surgical cricothyroidotomy
Tracheostomy
Mechanical ventilation
Optimal mechanical ventilation
Permissive hypercapnoea
Deliberate hyperventilation
Extubation in the emergency department
2.2 Oxygen therapy
Introduction
Uses of supplemental oxygen
 To correct defects in the delivery of inspired gas to the lungs. A clear airway is essential.
To correct defects in the delivery of inspired gas to the lungs. A clear airway is essential.
 Where there is inadequate oxygenation of blood due to defects in pulmonary gas exchange.
Where there is inadequate oxygenation of blood due to defects in pulmonary gas exchange.
 To provide 100% oxygen where clinically indicated.
To provide 100% oxygen where clinically indicated.
 To titrate oxygen dose in patients with impaired ventilatory response to carbon dioxide.
To titrate oxygen dose in patients with impaired ventilatory response to carbon dioxide.
Physiology of oxygen
Oxygen transport chain
Ventilation
Alveolar gas equation

Pulmonary gas exchange

 , ∝=proportional to, A=area of tissue, T=tissue thickness, Sol=solubility of the gas, MW=molecular weight, PA=alveolar partial pressure, and Ppa=pulmonary artery partial pressure.
, ∝=proportional to, A=area of tissue, T=tissue thickness, Sol=solubility of the gas, MW=molecular weight, PA=alveolar partial pressure, and Ppa=pulmonary artery partial pressure.
Expected A−a gradient

Oxygen carriage in the blood
 uptake of oxygen by haemoglobin (Hb)
uptake of oxygen by haemoglobin (Hb)
 generation of a cardiac output to carry the oxygenated haemoglobin to the peripheral tissues
generation of a cardiac output to carry the oxygenated haemoglobin to the peripheral tissues
 dissociation of oxygen from haemoglobin into dissolved oxygen in plasma
dissociation of oxygen from haemoglobin into dissolved oxygen in plasma
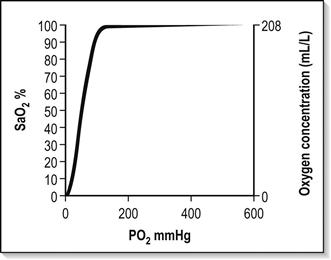
Haemoglobin–oxygen (Hb–O2) dissociation curve
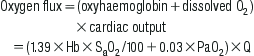
Oxygen flux
Local tissue perfusion and diffusion
Tissue utilization of oxygen
Oxygen delivery systems
Definitions
Variable-performance oxygen delivery systems
Fixed-performance oxygen delivery systems
One hundred per cent (100%) oxygen systems
General principles
Variable-performance systems
< div class='tao-gold-member'>
Related posts:
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree