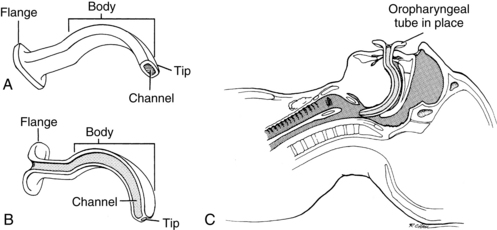
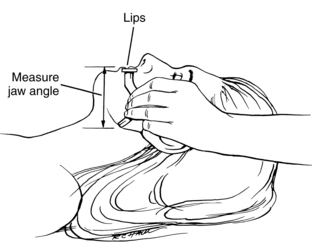
PROCEDURE 11 • Oropharyngeal airways are usually disposable and made of hard curved plastic. • Oral airways are inserted through the open mouth with the posterior tip resting in the patient’s pharynx. • The oral airway is placed over the tongue. The curvature or body of the airway displaces the tongue forward from the posterior pharyngeal wall, a common site of airway obstruction. • An oral airway has four parts: the flange, body, tip, and channel (Fig. 11-1). The flange, or flat surface, protruding from the mouth rests against the lips. This design protects against aspiration into the airway. The body of the airway curves over the tongue. The tip is the distal-most part of the airway toward the base of the tongue. The channel enables passage of a suction catheter. • The Guedel airway is tubular with a flattened-oval inner diameter. A suction catheter passes through the central lumen or channel. • The Berman airway has a channel on either side that guides the catheter along the edge of the airway into the pharyngeal space. • Oral airways are manufactured in a variety of lengths and widths for adults, children, and infants. Sizing depends on the age and size of the patient (Table 11-1). An alternative method used to select the size of an oral airway is to measure the airway by placing the flange alongside the patient’s lips and the oral airway tip alongside the angle of the jaw (Fig. 11-2). Improperly sized airways can cause airway obstruction (if they are too small) and tongue displacement against the oropharynx (if they are too large). TABLE 11-1 From Cummins RO, editor: Airway, airway adjuncts, oxygenation, and ventilation. In ACLS: principles and practice, Dallas, 2003, American Heart Association, 145. FIGURE 11-2
Oropharyngeal Airway Insertion
PREREQUISITE NURSING KNOWLEDGE
Size of Patient
Diameter of Oral Airway (mm)
Size of Oral Airway (Guedel)
Large adult
100
5
Medium adult
90
4
Small adult
80
3
Related posts:
![]() 69: Central Venous Catheter Site Care
69: Central Venous Catheter Site Care
![]() 49: Epicardial Pacing Wire Removal
49: Epicardial Pacing Wire Removal
![]() 100: Cervical Traction Maintenance
100: Cervical Traction Maintenance
![]() 136: Organ Donation: Identification of Potential Organ Donors, Request for Organ Donation, and Care of the Organ Donor
136: Organ Donation: Identification of Potential Organ Donors, Request for Organ Donation, and Care of the Organ Donor
![]() 38: Peripheral Nerve Stimulators
38: Peripheral Nerve Stimulators
![]() 130: Fecal Containment Devices and Bowel Management System
130: Fecal Containment Devices and Bowel Management System
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


11: Oropharyngeal Airway Insertion