CHAPTER 58
Temporomandibular Disorder
(TMD, TMJ Syndrome)
Presentation
Patients usually complain of poorly localized facial pain or headache that does not appear to conform to a strict anatomic distribution. The pain is generally dull and unilateral, centered in the temple above and behind the eye, and in and around the ear. The pain may be associated with mastication and passive movement of the mandible, instability of the temporomandibular joint (TMJ), crepitus, or clicking with movement of the jaw. It is often described as an earache.
Other less obvious symptoms include radiation of pain down the carotid sheath, tinnitus, dizziness, decreased hearing, itching, sinus symptoms, a foreign body sensation in the external ear canal, and trigeminal, occipital, and glossopharyngeal neuralgias.
Patients may have been previously diagnosed as suffering from migraine headaches, sinusitis, or recurrent external otitis. Predisposing factors include malocclusion, trauma, recent extensive dental work, or a habit of grinding the teeth (bruxism), all of which put unusual stress on the TMJ.
Clinical signs include tenderness of the chewing muscles, the ear canal, or the joint itself; restricted opening of the jaw or lateral deviation on opening; and a normal neurologic examination.
What To Do:
 The patient should be asked about TMJ pain with jaw motion, such as chewing or yawning. Determine if there is a history of jaw trauma or involvement of other joints (which may be indicative of an underlying rheumatologic disorder).
The patient should be asked about TMJ pain with jaw motion, such as chewing or yawning. Determine if there is a history of jaw trauma or involvement of other joints (which may be indicative of an underlying rheumatologic disorder).
 Examine the head thoroughly for other causes of the pain, including assessment of visual acuity, examination of the cranial nerves, and palpation of the scalp muscles and the temporal arteries.
Examine the head thoroughly for other causes of the pain, including assessment of visual acuity, examination of the cranial nerves, and palpation of the scalp muscles and the temporal arteries.
 The TMJ examination should focus on the joint and the muscles of mastication, with careful attention to whether palpation can reproduce the patient’s pain. While your fingers are firmly palpating the preauricular area, ask the patient to repeatedly open and close her mouth. This maneuver will be painful if the TMJ is the source of her pain. Intraoral palpation of the pterygoid muscles allows evaluation of spasm and tenderness of the muscle. The mandible can be distracted laterally by the patient to assess for pain during range of motion of the TMJ. Crepitus or a “click” may be heard or palpated with movement of the mandible. One should note, however, that given the prevalence of TMJ crepitance, the presence of these findings does not necessarily implicate the TMJ as the cause of the patient’s symptoms.
The TMJ examination should focus on the joint and the muscles of mastication, with careful attention to whether palpation can reproduce the patient’s pain. While your fingers are firmly palpating the preauricular area, ask the patient to repeatedly open and close her mouth. This maneuver will be painful if the TMJ is the source of her pain. Intraoral palpation of the pterygoid muscles allows evaluation of spasm and tenderness of the muscle. The mandible can be distracted laterally by the patient to assess for pain during range of motion of the TMJ. Crepitus or a “click” may be heard or palpated with movement of the mandible. One should note, however, that given the prevalence of TMJ crepitance, the presence of these findings does not necessarily implicate the TMJ as the cause of the patient’s symptoms.
 Muscular trigger points that reproduce or intensify the patient’s pain on firm palpation indicate a myofascial origin that may benefit from a trigger point injection (see Chapter 123). Look for signs of bruxism, such as ground-down teeth, and percuss the teeth to possibly elicit dental pain as the source of the patient’s discomfort.
Muscular trigger points that reproduce or intensify the patient’s pain on firm palpation indicate a myofascial origin that may benefit from a trigger point injection (see Chapter 123). Look for signs of bruxism, such as ground-down teeth, and percuss the teeth to possibly elicit dental pain as the source of the patient’s discomfort.
 If the patient has a headache, perform a complete neurologic examination, including funduscopy. If the temporal artery is tender, swollen, or inflamed, send blood to be tested for an erythrocyte sedimentation rate (see Chapters 6 and 9).
If the patient has a headache, perform a complete neurologic examination, including funduscopy. If the temporal artery is tender, swollen, or inflamed, send blood to be tested for an erythrocyte sedimentation rate (see Chapters 6 and 9).
 Complete evaluation of TMJ disorders, in addition to a thorough physical examination, includes panoramic or plain radiographs and can include MRI studies. These imaging studies can be deferred until it is clear that symptoms are not resolving after 3 to 4 weeks of conservative therapy.
Complete evaluation of TMJ disorders, in addition to a thorough physical examination, includes panoramic or plain radiographs and can include MRI studies. These imaging studies can be deferred until it is clear that symptoms are not resolving after 3 to 4 weeks of conservative therapy.
 If the pain is severe and clearly isolated to the joint, try an injection into the TMJ, just anterior to the tragus, with 1 to 2 mL of plain lidocaine 1% (Xylocaine) or bupivacaine 0.5% (Marcaine). If symptoms have been prolonged, you can combine this with 10 mg (0.25 mL) of methylprednisolone (Depo-Medrol) (Figure 58-1). If this helps, the diagnosis may have been made, and if a steroid was given, long-term relief may have been provided.
If the pain is severe and clearly isolated to the joint, try an injection into the TMJ, just anterior to the tragus, with 1 to 2 mL of plain lidocaine 1% (Xylocaine) or bupivacaine 0.5% (Marcaine). If symptoms have been prolonged, you can combine this with 10 mg (0.25 mL) of methylprednisolone (Depo-Medrol) (Figure 58-1). If this helps, the diagnosis may have been made, and if a steroid was given, long-term relief may have been provided.
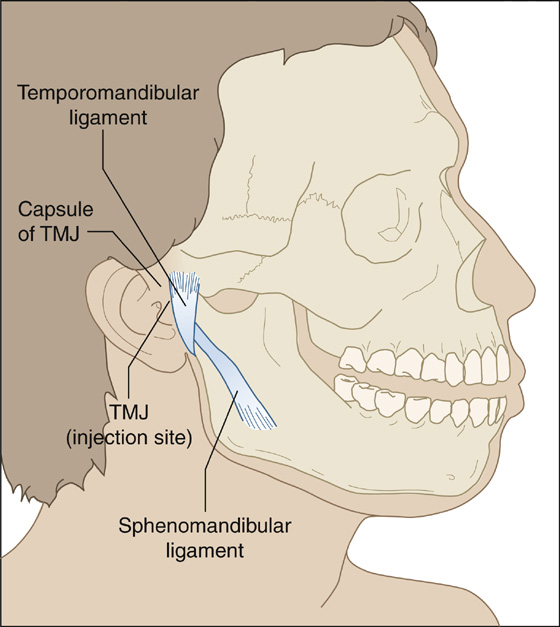
Figure 58-1 Proper temporomandibular joint (TMJ) injection site.
 Explain to the patient the pathophysiology of the syndrome, including how many different symptoms may be produced by inflammation at one joint, how TMJ pain is not necessarily related to arthritis at other joints, and how common it is (some estimates are as high as 20% of the population).
Explain to the patient the pathophysiology of the syndrome, including how many different symptoms may be produced by inflammation at one joint, how TMJ pain is not necessarily related to arthritis at other joints, and how common it is (some estimates are as high as 20% of the population).
 Prescribe anti-inflammatory analgesics (e.g., ibuprofen, naproxen), a soft diet, application of heat, and muscle relaxants (e.g., metaxalone [Skelaxin]) if necessary for muscle spasm. Application of ice can also be comforting.
Prescribe anti-inflammatory analgesics (e.g., ibuprofen, naproxen), a soft diet, application of heat, and muscle relaxants (e.g., metaxalone [Skelaxin]) if necessary for muscle spasm. Application of ice can also be comforting.
 Have the patient avoid extreme jaw movements, such as yawning, yelling, and singing as well as chewing (especially gum or ice).
Have the patient avoid extreme jaw movements, such as yawning, yelling, and singing as well as chewing (especially gum or ice).
 If the symptoms do not clear after 2 to 4 weeks, refer the patient for follow-up with a dentist or an otolaryngologist who has some interest in and experience with TMJ problems. Long-term treatments include orthodontic correction, physical therapy, and, sometimes, psychotherapy and treatment with antidepressants. Surgical intervention should be a last resort. Earlier follow-up should be provided if symptoms dramatically worsen or change.
If the symptoms do not clear after 2 to 4 weeks, refer the patient for follow-up with a dentist or an otolaryngologist who has some interest in and experience with TMJ problems. Long-term treatments include orthodontic correction, physical therapy, and, sometimes, psychotherapy and treatment with antidepressants. Surgical intervention should be a last resort. Earlier follow-up should be provided if symptoms dramatically worsen or change.
What Not To Do:
 Do not rule out TMJ arthritis simply because the joint is not tender on examination. This syndrome typically fluctuates, and the diagnosis often is made based on the history alone.
Do not rule out TMJ arthritis simply because the joint is not tender on examination. This syndrome typically fluctuates, and the diagnosis often is made based on the history alone.
 Do not omit examining the TMJ in the workup of any headache or earache.
Do not omit examining the TMJ in the workup of any headache or earache.
 Do not administer narcotics unless there is going to be early follow-up.
Do not administer narcotics unless there is going to be early follow-up.
Discussion
Painful disorders of the temporomandibular joint involve the trigeminal nerve. Other areas innervated by the trigeminal nerve help explain referred pain from the TMJ. Included are the dura mater, orbit, paranasal sinuses, tympanic membrane, and oral cavity and teeth, which help explain headaches, eye pain, sinus pressure, otalgia, and dental pain, respectively.
The muscles of mastication are abductors (jaw opening) and adductors (jaw closing) muscles. The temporalis, masseter, and medial pterygoids are adductors, whereas the lateral pterygoids are the primary abductors of the jaw.
The relative causative roles of abnormal joint anatomy, inadequate dentition, unsatisfactory occlusion, bruxism, dysfunction of the masticatory muscles, and emotional disorders remain controversial. To stress the role played by muscles, it has been suggested that the term myofascial pain dysfunction syndrome is more accurate than the term TMJ arthritis. Both these terms, as well as TMJ syndrome, are now considered to be outdated. The term temporomandibular joint disorder (TMD) is an umbrella term that combines a true disorder of the TMJ with involvement of the muscles of mastication. There is also much debate as to the indications for and the efficacy of treatment modalities aimed at these presumed causes. At the least, irreversible treatments such as surgery should be replaced by more conservative therapy. The use of bite blocks for bruxism was based on outdated information and may serve only to alter normal dental occlusion, with deleterious effects.
Perhaps everyone suffers pain in the TMJ occasionally, and only a few require treatment or modification of lifestyle to reduce symptoms. In the emergency department or urgent care clinic, the diagnosis of TMJ pain is often suspected but seldom made definitively. It can be gratifying, however, to see patients with a myriad of seemingly unrelated symptoms respond dramatically after only conservative measures and advice are offered.
It is worth noting that a study of approximately 450 patients with TMJ pain demonstrated otalgia to be the presenting complaint in 48%. In this study, the TMD (and hence otalgia) was successfully managed with conservative therapies, such as heat, massage, patient education, occlusal splints, and pain control.
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


