CHAPTER 61
Lateral Femoral Cutaneous Nerve Block
INTRODUCTION
The lateral femoral cutaneous nerve (LFCN) is a purely sensory nerve from the lumbar plexus and is derived from the L2-L3 nerve roots. LFCN pain is believed to be associated with obesity, pregnancy, or a constricting belt. Symptoms are thought to be due to entrapment of the LFCN as it passes through or under the inguinal ligament. The LFCN is also at risk of irritation from bone graft due to the nerves close proximity to the iliac crest. Because it is a sensory nerve, symptoms after injury, irritation, or laceration to the LFCN include dysaesthetic pain, numbness and paresthesias localized or radiating to the buttocks or anterolateral thigh. The lateral femoral cutaneous nerve innervates the skin on the lateral part of the thigh and because it is 1 of the 6 nerves that comprise the lumbar plexus, the LFC can be blocked as part of the lumbar plexus block or on occasion with a femoral nerve block.
INDICATIONS
• Diagnosing and treating nerve entrapment (meralgia paresthetica)
• Regional aesthesia
![]() Skin grafting from the upper thigh
Skin grafting from the upper thigh
![]() Muscle biopsy
Muscle biopsy
• Postoperative analgesia after hip surgery
• Repeated blocks can function as a treatment for meralgia paresthetica
• Predicting outcome of neuromodulation techniques or surgical neurolysis
RELEVANT ANATOMY
• The lateral femoral cutaneous nerve of the thigh is 1 of the 6 nerves of the lumbar plexus. It arises from the posterior division of the second and third lumbar nerves.
• The nerve traverses the psoas muscle and emerges alone from the lateral aspect of the muscle.
• After crossing the psoas muscle, the lateral femoral cutaneous nerve follows an oblique and lateral course between the iliac muscle and the fascia iliaca in the direction of the anterosuperior iliac spine (ASIS).
• At this point, it provides branches for the peritoneum. It then enters the thigh by passing through or under the inguinal ligament and over the sartorius muscle, where it bifurcates into an anterior and posterior branch (Figure 61-1).
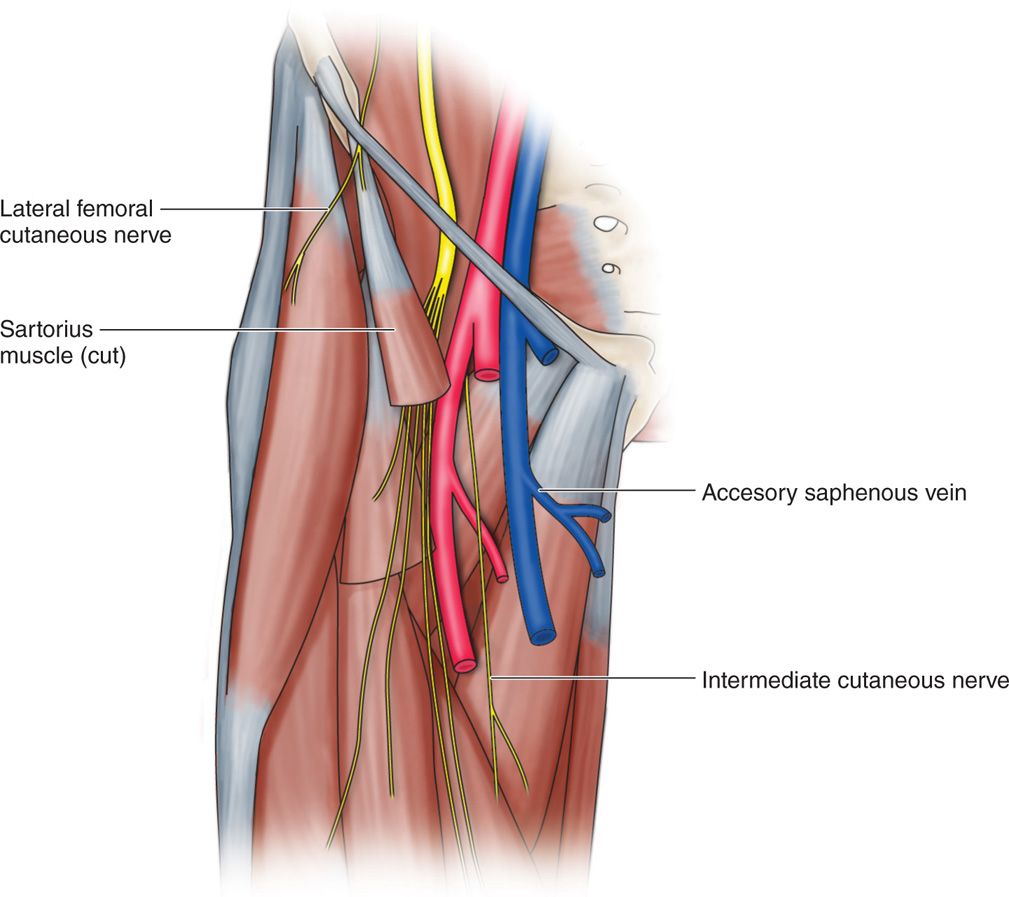
Figure 61-1. Dissection of the anterior thigh anatomy depicting the location of the LCFN.
• The anterior branch supplies the anterolateral part of the thigh as far as the knee. It emerges approximately 10 cm below the inguinal ligament.
The distal most fibers communicate with the anterior cutaneous branches of the femoral nerve and the infrapatellar branches of the saphenous nerve creating the peripatellar plexus. The posterior branch pierces the tensor fascia lata and supplies the skin of the superior and lateral aspects of the thigh from the greater trochanter to the middle of the thigh (Figure 61-2).
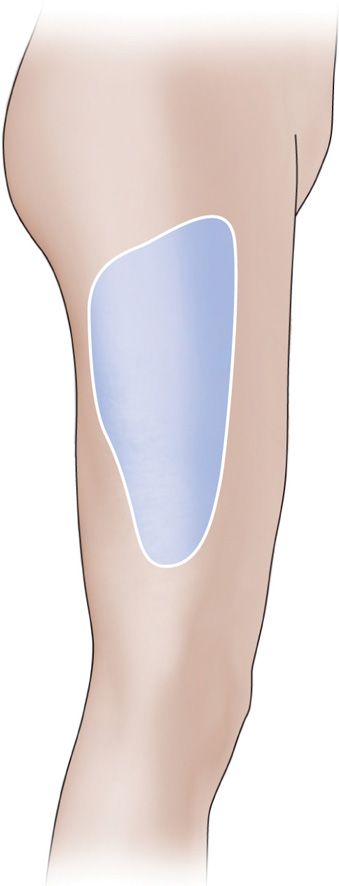
Figure 61-2. Cutaneous distribution of the LFCN.
Anatomical variations that may explain failure of anesthesia after a femoral nerve block:
• Described in 25% of cases
• Arise directly from the femoral nerve in 18% of cases
• LFCN innervation may extend medially as far as the anterior surface of the thigh in 31% of cases.
CONTRAINDICATIONS
• Infection, systemic or localized
• Coagulopathy (relative contraindication)
• Allergy to the injectate
For patients with a coagulopathy a 27-gauge needle is recommended. Meralgia paresthetica refractory to the injection and other causes of lateral thigh pain need to be investigated. Differential diagnosis are fractures of the anterior superior iliac spine, iliac bone graft, pelvic tumor, psoas tumor, lumbar metastasis, tight pants, seat belt trauma, waist belts, hip arthroplasty, and obesity. The risks and benefits of the procedure need to be explained to the patient thoroughly before the procedure.
PREOPERATIVE CONSIDERATIONS
• Informed consent including the risks and benefits of the procedure and all reasonably anticipated complications.
• Anticoagulation is not a significant concern for an injection in this location.
• Examine the region for infection, cutaneous lesions, hip pathology, and other inguinal pathology.
• Patient must be able to lay be supine for the length of the procedure.
• Be sure that all equipment is operational.
Equipment
Materials
• Marking pen
• Sterile gloves
• Sterile bandage
• 3-cc syringe with 25-gauge needle for cutaneous anesthetic injection
• 10-cc syringe for injectate
• 22- or 25-gauge 1.5- or 3-in insulated needle appropriate for injecting with peripheral nerve stimulation
• Fluoroscopy or ultrasound for needle guidance
• Nerve stimulator
Medications
• 1 cc 1% lidocaine for skin numbing
• 1 cc of 40 mg/cc of methylprednisolone acetate or triamcinolone acetonide (Depo Medrol or Kenalog) for injectate
• 6 cc of 1% lidocaine or 0.5% marcaine for injectate
Positioning of the Patient
The patient should be supine with the thigh in neutral position.
Intraprocedural Technical Steps
The Fanning Technique
• This is a common technique used for the lateral femoral cutaneous nerve block.
• Patient should be in supine position; an area 2 cm medial and 2 cm caudal from the anterior superior iliac spine (ASIS) is marked (Figure 61-3).

Figure 61-3. Right lateral femoral cutaneous nerve localization and injection. (Reproduced with permission from Hadzic A: The New York School of Regional Anesthesia Textbook of Regional Anesthesia and Acute Pain Management: http://www.accessanesthesiology.com. Copyright © The McGraw-Hill Companies, Inc. All rights reserved.)
• Sterile preparation of the area in usual fashion.
• A skin wheal can be performed, although it is not necessary as most patients tolerate the procedure well without the wheal.
• A 25-gauge 1.5-in needle is inserted at the target site and advanced until a loss of resistance or a “pop” is felt when needle pierces the fascia lata.
• The anesthetic/corticosteroid mixture is injected.
• The needle is removed and a Band-Aid is applied.
• Local anesthetic alone can be used for diagnostic purposes.
The Transinguinal Technique
• This is another technique that can be used to block the lateral femoral cutaneous nerve.
• Palpate the most medial part of the anterior superior iliac spine and mark a point 1 cm medial to the ASIS.
• Then extend a vertical line caudally just below the inguinal ligament to determine the site of introduction of the needle (Figure 61-3).
• Prepare the site with povidone iodine (Betadine) or chlorhexidine gluconate (Chloraprep) antiseptic solution.
• A 50-mm insulated needle connected to a nerve stimulator (1.5 mA, 2 Hz, 0.3 ms) is introduced perpendicular to the skin until paresthesia on the lateral border of the thigh is elicited.
• The needle position is adjusted to maintain the paresthesia with a current of 0.5 mA.
• After negative aspiration for blood, the anaesthetic/corticosteroid mixture is slowly injected.
• The needle is removed and a Band-aid is applied.
Ultrasound guidance with or without nerve stimulation can be used to further ensure the localization of the needle placement (Figure 61-4). Fluoroscopic confirmation with a neurogram can be obtained, but usually does not enhance the efficacy of the injection.
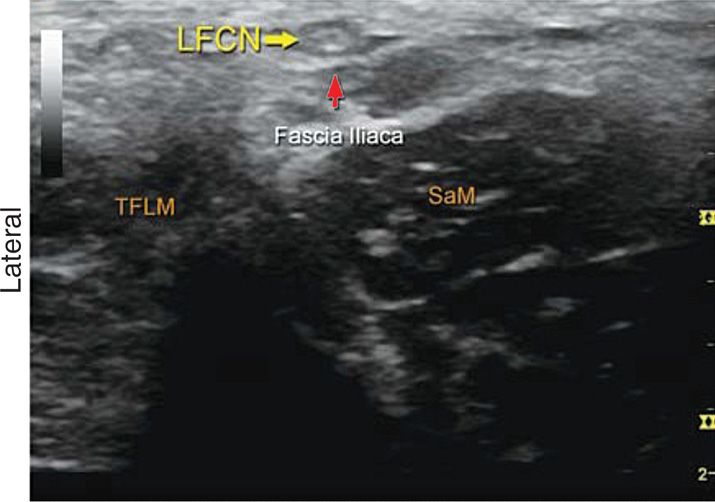
Figure 61-4. Transverse ultrasound image of the lateral femoral cutaneous nerve (LFCN). (Reproduced with permission from Hadzic A: Hadzic’s Peripheral Nerve Blocks and Anatomy for Untrasound-Guided Regional Anesthesia, 2nd Edition: www.accessanesthesiology.com. Copyright © The McGraw-Hill Companies, Inc. All rights reserved.)
Potential Complications
• Intravascular injection
• Local anesthetic toxicity (central nervous system and cardiovascular toxicity)
• LFCN trauma resulting in transient neuritis or permanent injury
• Transient femoral nerve block resulting in prolonged motor blockade of the muscles of the thigh
• Hematoma formation
• Block failure
POSTPROCEDURE CONSIDERATIONS
Examination postprocedure is necessary to assess for anesthesia to the region of the lateral thigh innervated by the LFCN. Quadriceps weakness in both hip flexion and knee extension needs to be assessed. Precautions toward ambulation and driving need to be emphasized for any prolonged anesthetic response.
CLINIC PEARLS AND PITFALLS
• This injection can be both diagnostic and therapeutic.
• This procedure can be performed without nerve stimulation, radiographic or ultrasound guidance6 but the use of the nerve stimulator does not increase the success rate of obtaining adequate neural blockade.7
• With a successful block, there should be anesthesia of the upper two-thirds of the anterolateral thigh.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


