Cervical Plexus Block
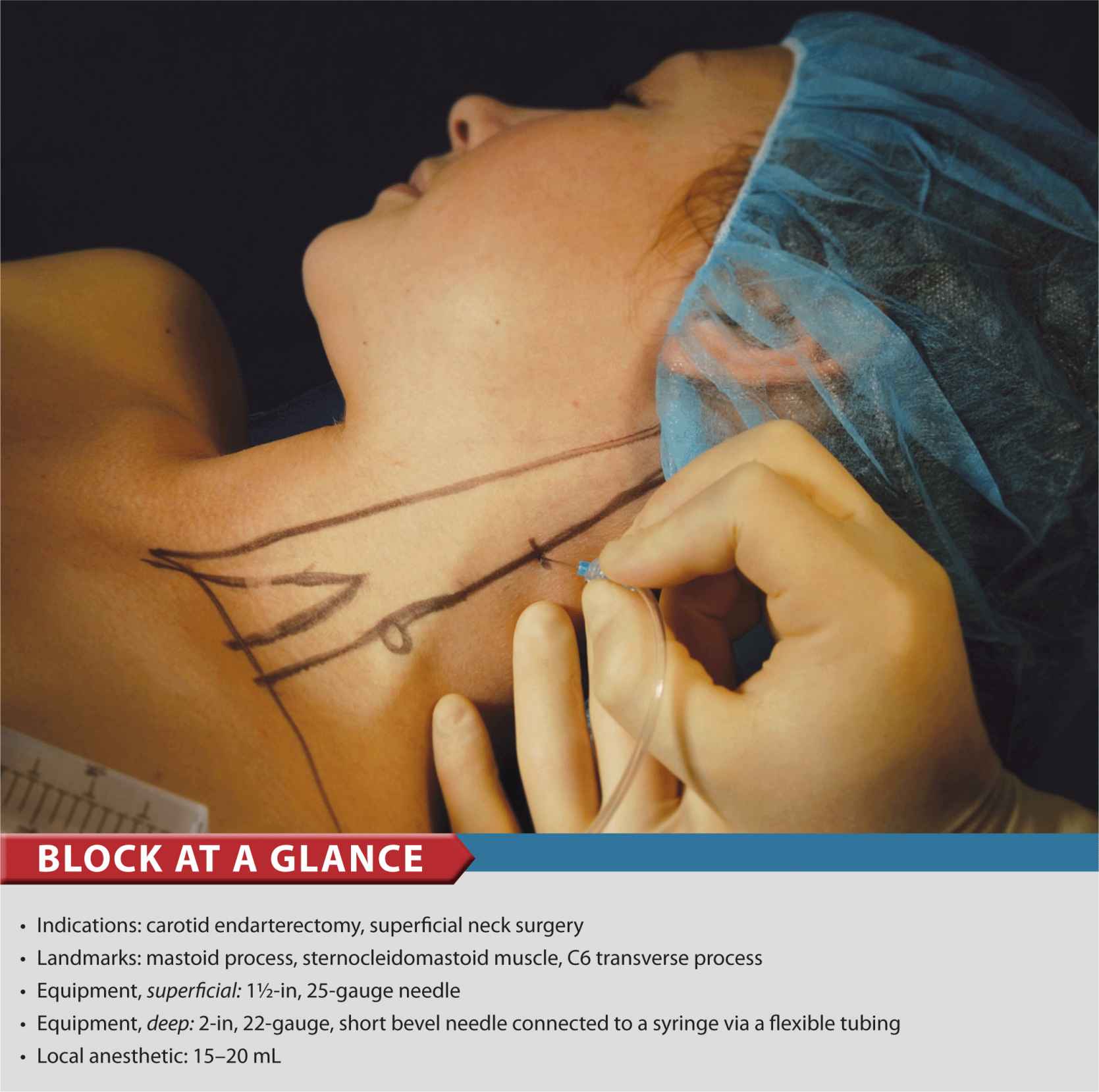
FIGURE 11-1. Needle insertion for superficial cervical plexus block. The needle is inserted behind the posterior border of the sternocleidomastoid muscle.
General Considerations
Cervical plexus block can be performed using two different methods. One is a deep cervical plexus block, which is essentially a paravertebral block of the C2-4 spinal nerves (roots) as they emerge from the foramina of their respective vertebrae. The other method is a superficial cervical plexus block, which is a subcutaneous blockade of the distinct nerves of the anterolateral neck. The most common clinical uses for this block are carotid endarterectomy and excision of cervical lymph nodes. The cervical plexus is anesthetized also when a large volume of local anesthetic is used for an interscalene brachial plexus block. This is because local anesthetic invariably escapes the interscalane groove and layers out underneath the deep cervical fascia where the branches of the cervical plexus are located.
The sensory distribution for the deep and superficial blocks is similar for neck surgery, so there is a trend toward favoring the superficial approach. This is because of the potentially greater risk for complications associated with the deep block, such as vertebral artery puncture, systemic toxicity, nerve root injury, and neuraxial spread of local anesthetic.
Functional Anatomy
The cervical plexus is formed by the anterior rami of the four upper cervical nerves. The plexus lies just lateral to the tips of the transverse processes in the plane just behind the sternocleidomastoid muscle, giving off both cutaneous and muscular branches. There are four cutaneous branches, all of which are innervated by roots C2-4. These emerge from the posterior border of the sternocleidomastoid muscle at approximately its midpoint, and they supply the skin of the anterolateral neck (Figures 11-2 and 11-3). The second, third, and fourth cervical nerves typically send a branch each to the spinal accessory nerve or directly into the deep surface of the trapezius to supply sensory fibers to this muscle. In addition, the fourth cervical nerve may send a branch downward to join the fifth cervical nerve and participates in formation of the brachial plexus. The motor component of the cervical plexus consists of the looped ansa cervicalis (C1-C3), from which the nerves to the anterior neck muscles originate, and various branches from individual roots to posterolateral neck musculature (Figure 11-4). The C1 spinal nerve (the suboccipital nerve) is strictly a motor nerve, and is not blocked with either technique. One other significant muscle innervated by roots of the cervical plexus includes the diaphragm (phrenic nerve, C3,4,5) (Table 11-1).
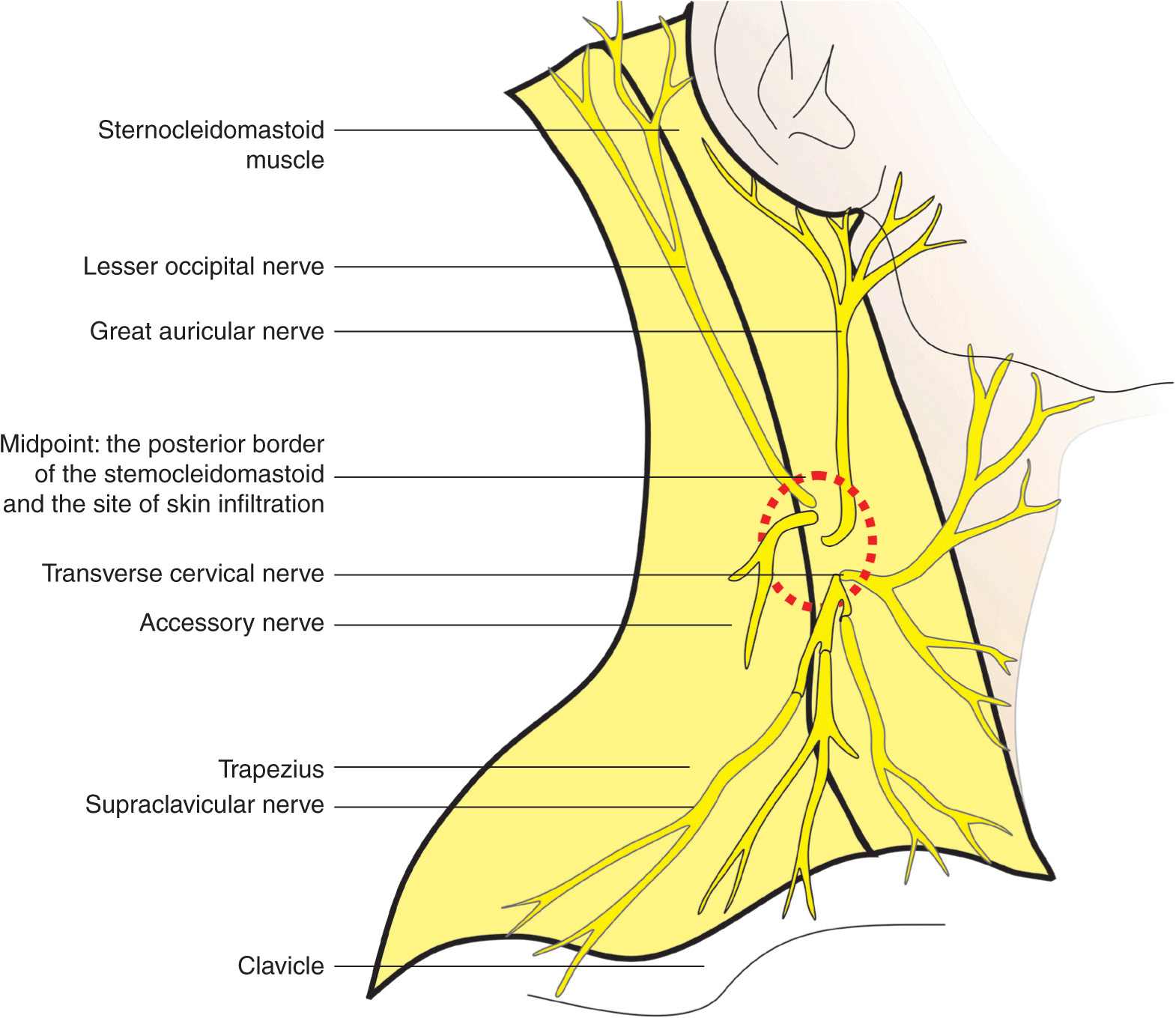
FIGURE 11-2. The superficial cervical plexus and its terminal nerves. Anatomy of the superficial cervical plexus and its branches are shown emerging behind the posterior border of the sternocleidomastoid muscle.
FIGURE 11-3. Anatomy of the superficial cervical plexus. ![]() Sternocleidomastoid muscle
Sternocleidomastoid muscle ![]() mastoid process
mastoid process ![]() clavicle
clavicle ![]() external jugular vein.
external jugular vein.
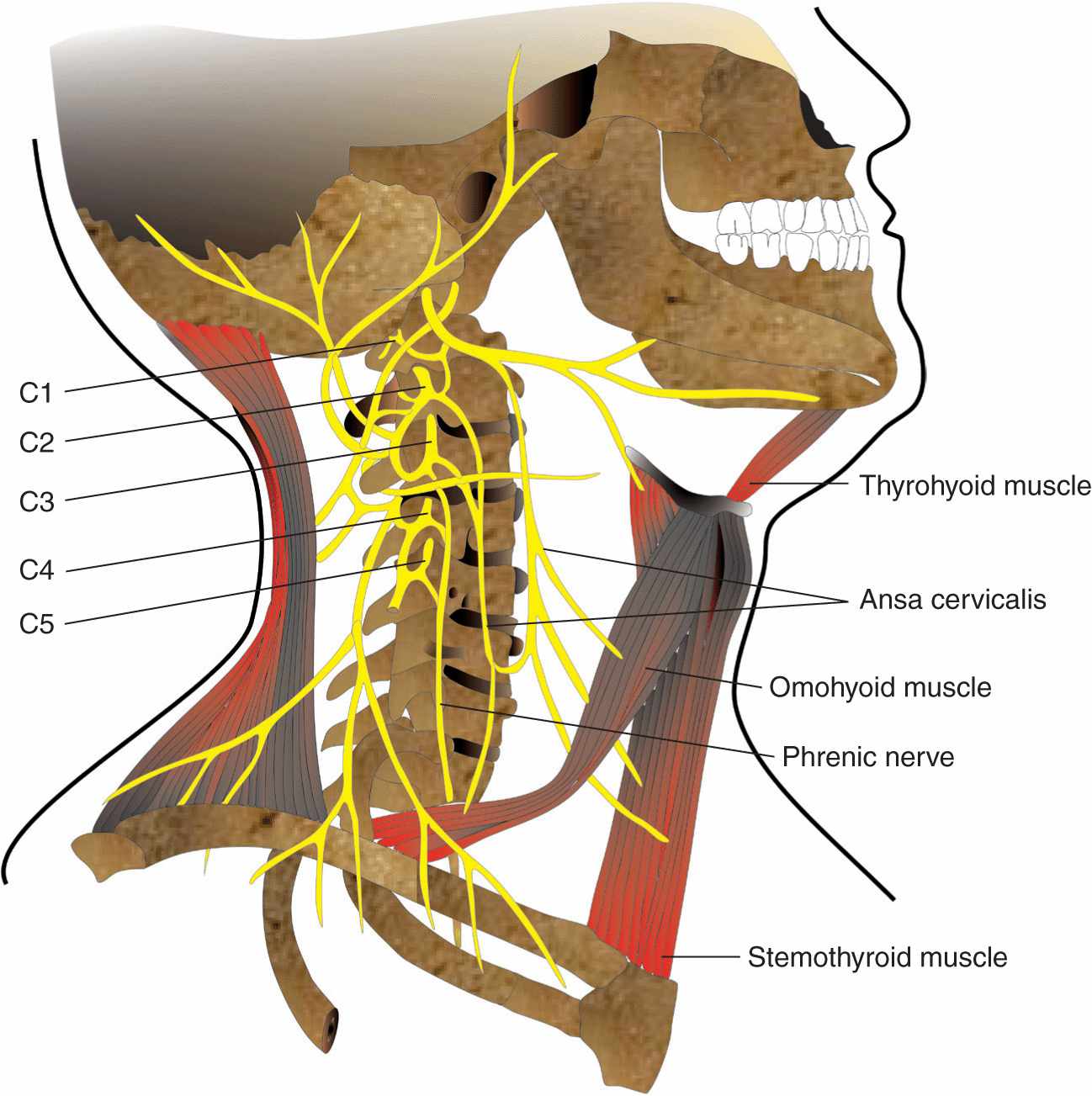
FIGURE 11-4. The roots origin of the cervical plexus.
TABLE 11-1 Cervical Plexus
Distribution of Blockade
Cutaneous innervation of both the deep and the superficial cervical plexus blocks includes the skin of the anterolateral neck and the ante- and retroauricular areas (Figure 11-5). In addition, the deep cervical block anesthetizes three of the four strap muscles of the neck, geniohyoid, the prevertebral muscles, sternocleidomastoid, levator scapulae, the scalenes, trapezius, and the diaphragm (via blockade of the phrenic nerve).
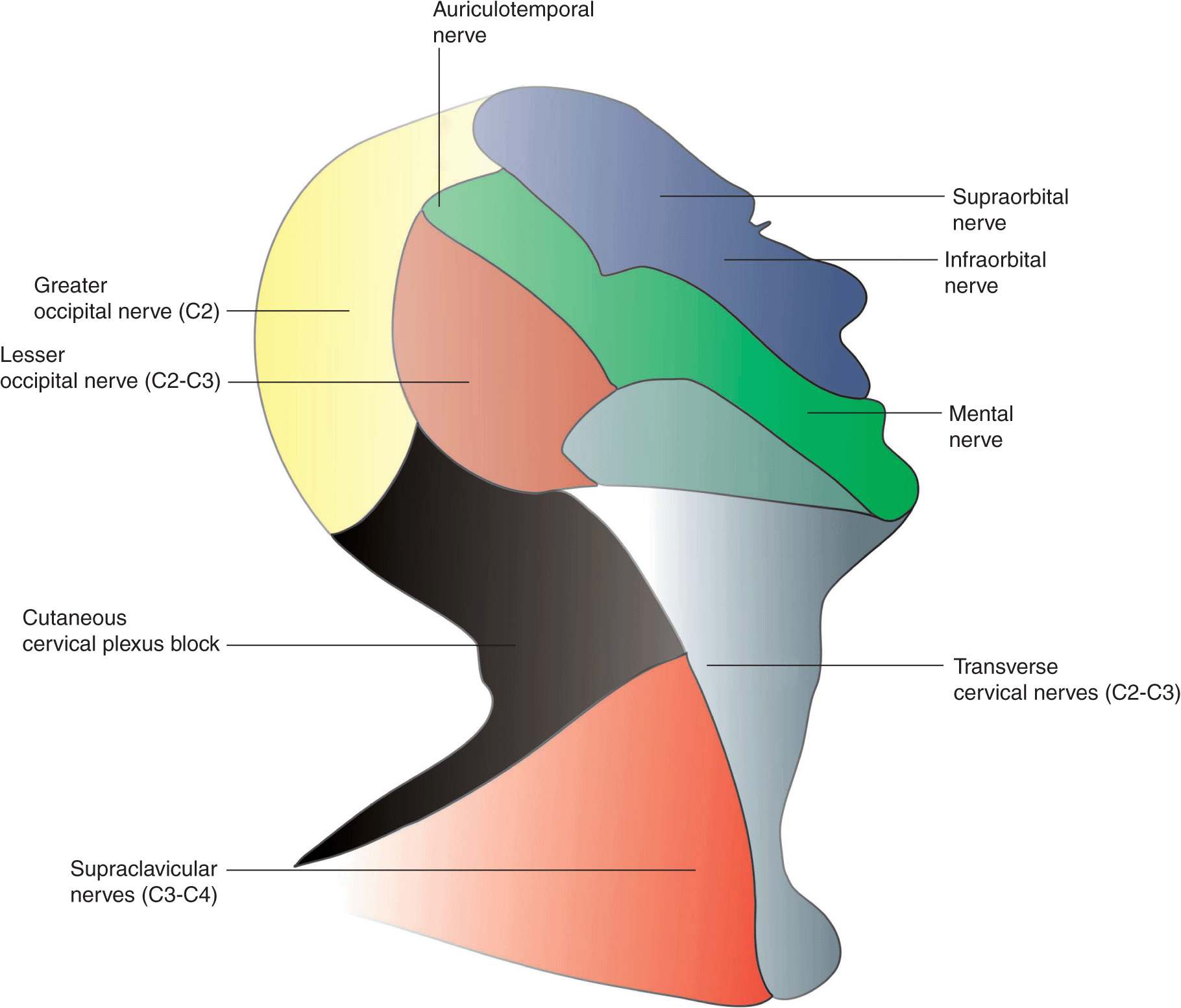
FIGURE 11-5. Sensory innervation of the lateral aspect of the head and neck and contribution of the superficial cervical plexus.
Superficial Cervical Plexus Block
Equipment
A standard regional anesthesia tray is prepared with the following equipment:
• Sterile towels and gauze packs
• A 20-mL syringe with local anesthetic, attached to a 1½-in, 25-gauge needle, typically via a flexible tubing
• Sterile gloves, marking pen
Landmarks and Patient Positioning
The patient is in a supine or semi-sitting position with the head facing away from the side to be blocked. These are the primary landmarks (Figure 11-6) for performing this block:
FIGURE 11-6. Surface landmarks for superficial cervical plexus block. White dot: insertion of the clavicular head of the sternocleidomastoid muscle. Blue dot: Mastoid process. Uncolored circle: Transverse process of C6 vertebrate. Red dot: Needle insertion site at the midpoint between C6 and mastoid process behind the posterior border of the sternocleidomastoid muscle.
1. Mastoid process
2. Clavicular head of the sternocleidomastoid
3. The midpoint of the posterior border of the sternocleidomastoid (this is aided by identifying the first two landmarks)
Maneuvers to Facilitate Landmark Identification
The sternocleidomastoid muscle can be better differentiated from the deeper neck structures by asking the patient to raise their head off the table.
Technique
After cleaning the skin with an antiseptic solution, the needle is inserted along the posterior border of the sternocleidomastoid, and three injections of 5 mL of local anesthetic are injected behind the posterior border of the sternocleidomastoid muscle subcutaneously, perpendicularly, cephalad, and caudad in a “fan” fashion (Figure 11-7).
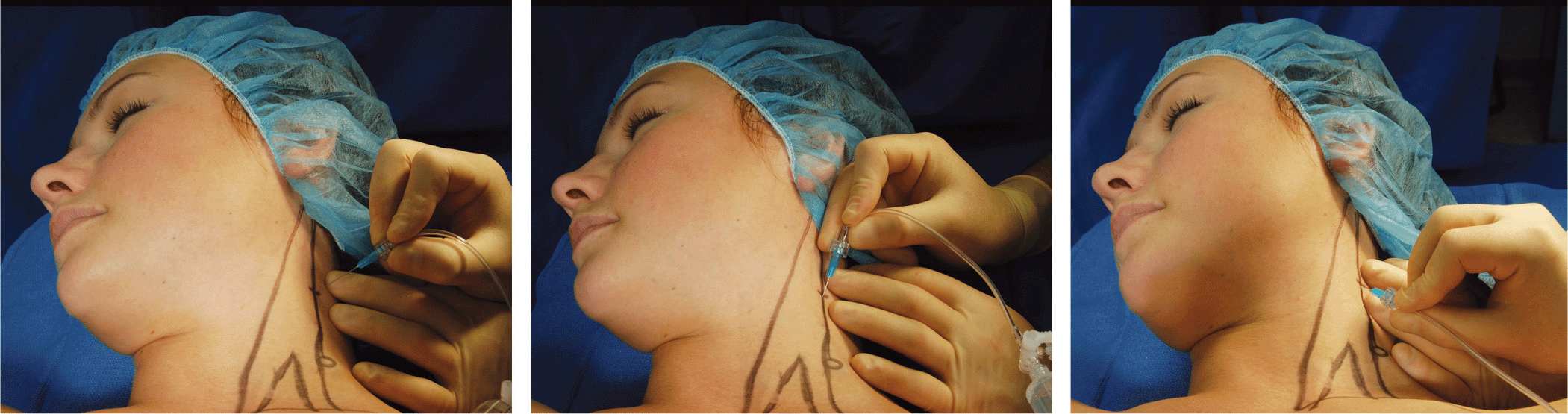
FIGURE 11-7. Injection of local anesthetic for superficial cervical plexus. The injection is made fan-wise behind the posterior border of the sternocleidomastoid muscle at a depth of approximately 1 cm in average-size patients.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


